
Episode 088: Disorganized Attachment: Fear Without Solution Part 2
By listening to this episode, you can earn 1 Psychiatry CME Credits.
Other Places to listen: iTunes, Spotify
Article Authors: Annabel Kuhn, BA, David Puder, MD
There are no conflicts of interest for this episode.
Understanding disorganized attachment as medical professionals is important because some patients have experienced trauma, or 2nd generation influences of trauma, which leads to this issue. As we continue to explore disorganized attachment and how we can help patients with this attachment style, it’s important to remember that this information provides the foundation for why empathy, connection, and emotion mirroring is vital in psychotherapy and psychiatry. Even though dissociation is a main feature of people who continue to have a disorganized attachment style later on in adolescence/adulthood, it’s not the only cause of dissociation. Childhood trauma of various kinds could create disorganized attachment and/or dissociation.
If you missed part one of disorganized attachment, the last podcast and article, read it first for a more complete picture of this attachment style.
Issues associated with disorganized attachment style
Attention Problems
It was previously thought that there was no association between disorganized attachment and ADHD (attention deficit hyperactivity disorder) (Faraone 1998), but a 2019 meta-analysis of 62 studies showed that children with disorganized attachment had more attention problems compared to children with organized attachment (r= 0.27) (Pallini 2019).
Studies regarding disorganized versus organized attachment and attention problems showed significant heterogeneity, Q (21) = 90.19, p < .001, I2 = 76.72. Risk status was a significant moderator: “The ES for at-risk disorganized children was higher than that for not at-risk children (p < .001)” (Pallini 2019)
“Risk was coded when children had clinical problems, suffered maltreatment/abuse, were adopted, or were children of adolescent parents, addicted parents, and/or parents with a previous stillbirth” (Pallini 2019)
Effect size for at-risk disorganized children: r = .35
Effect size for not at-risk children r = .15
Attention problems may be prevalent amongst individuals with disorganized attachment, and it’s important to keep this in mind when evaluating patients who may be experiencing disorganized attachment or focus issues. When patients come in who have focus issues, there may be factors other than ADHD involved and, when treated, the focus issues improve. It’s imperative that we give people the proper therapy for the root problems, not just the symptoms.
Problems Regarding Convergence in Parent-youth Reports of Adolescent Psychopathology
Convergence in parent-youth reports of adolescent psychopathology is critical for treatment planning. According to a 2019 study, “compared with organized adolescents, disorganized adolescents had lower parent–youth convergence in reports of their internalizing symptoms and higher convergence in reports of their externalizing symptoms” (Borelli 2019).
Externalizing symptoms = overactivity, poor impulse control, aggression, and noncompliance.
Internalizing symptoms = anxiety, sadness, social withdrawal, fearfulness.
So this study basically shows that parents' awareness of their disorganized adolescent’s internalizing symptoms are not in congruence with the adolescent’s self-reported internalizing symptoms.
What are possible explanations for this discrepancy?
Disorganized adolescents may have decreased awareness of their own internalizing symptoms.
There is a lack of communication regarding internal states to parents.
If the child was more of the disorganized type, the parent would have less of a clue of what was going on internally. They wouldn’t understand that the child was anxious, sad or fearful. This shows that there is usually a lack of mentalization from the parent as well as a lack of communication from the child.
Psychopathy and/or Violent Behavior
As discussed in part 1, disorganized attachment is associated with callous-unemotional traits at age 8. Callous-unemotional traits are associated with conduct disorder and perhaps a later development of antisocial personality disorder and/or psychopathy.
In fact, a 2014 study found that participants who obtained the highest PCL-R (Psychopathy Checklist-Revised) scores also showed indicators of disorganized attachment (using the Adult Attachment Interview, AAI) (Schimmenti 2014).
Participants: 139 Italian offenders who were convicted of violent crimes (murder, rape, child sexual abuse, armed robbery, assault causing bodily harm) were administered PCL-R. Qualitative analysis was performed on the transcripts of the ten participants who had the highest PCL-R scores, and when appropriate, coders used AAI (Adult Attachment Interview) to score “attachment states of mind”, and ASI (Attachment Style Interview) scales to score “attachment styles”
There were indicators of disorganized and/or dual attachment in 7 cases.
For example, transcripts showed “competitive internal working models of attachment including both anxious/preoccupied and avoidant/dismissing attitudes, and/or unresolved abuse and unresolved loss” (Schimmenti 2014)
“The investigation of attachment experiences in the subsample of the most severe psychopaths, who showed very high average scores on the items denoting devaluation of attachment bonds, further suggested that insecure and disorganized attachment styles and representations are very common among violent offenders, and that adverse childhood environments likely play a relevant role in the development of psychopathic personalities, as indicated by early studies on psychopathy and confirmed by some recent empirical evidence (Craparo et al. 2013; Frodi et al. 2001; Lang et al. 2002)” (Schimmenti 2014)
This is not to say that all people with disorganized attachment are going to be psychopaths. But, this study shows that the most severe psychopaths have large overlaps with attachment issues. Psychopaths are cold, calloused, and tend to have hundreds of sexual partners. Psychopaths see other human beings as an insect unworthy of connection. It’s interesting that it showed that people who score higher on the psychopathy checklist also have more of a disorganized attachment style.
Higher BMI
A 2019 study found that “attachment disorganized individuals are especially likely to engage in uncontrolled eating behaviours that are associated with a higher BMI (body mass index)” (Wilkinson 2019).
Parallel multiple mediation analysis (PROCESS) showed that uncontrolled eating (but not emotional eating or cognitive restraint) significantly mediated a relationship between disorganized attachment and body mass index. The article provides an explanation for why disorganized attachment relates to BMI as a result of uncontrolled eating behaviors: “these behaviors serve to affect regulatory need. Specifically, whilst the motivator for eating might not be emotion, it is some other eating-related cue, the incidental reward associated with such eating behaviors may have the unintended consequence of regulating affect” (Wilkinson 2019).
Uncontrolled eating behavior is consistent with disorganized attachment in two ways:
Disorganized attachment is associated with problematic regulation of anger and hostile emotions
When experienced, these emotions are associated with impulsivity which precipitates a need for affect regulation
Disorganized individuals are likely to receive less social support. Therefore, external forms of affect regulation, such as disinhibition of food consumption, may be one of the few ways a disorganized individual can manage his or her emotions
Incoherence is characteristic of disorganized attachment strategy and “specifically, it is likely that regulatory effects of uncontrolled eating behaviors are reinforced but have failed to be translated into a coherent strategy such as ‘emotional eating’” (Wilkinson 2019).
Disorganized attachment is important for clinicians to recognize and treat because according to the CDC, the prevalence of childhood obesity in the United States is 18.5% and affects about 13.7 million children and adolescents, and are therefore at risk for poor health. Preventing, recognizing, and treating disorganized attachment behaviors could conceivably improve this particular national health crisis.
Are There Genetic/Intrinsic Bases For Disorganized Attachment?
The studies that we have found accurately show how research develops. For example, during COVID-19, there is a big hydroxychloroquine debate because of a positive study early on, but later studies showed different results. This is an important example of how research develops. As we continue research, there may be more evidence to support a different perspective, but, as researchers, we do our best to look at the current data available and try to weigh in on whether the most recent data is stronger than the previous data. In that same way, as we learn more about disorganized attachment, we can understand what causes it, the predictors for it, and how to treat it.
Is There a Genetic Basis for Disorganized Attachment?
There are several genes that were previously thought to correspond to disorganized-attachment behavior, but more recent research says otherwise. Disorganized-attachment behavior is caused by multiple factors and has yet to be fully boiled-down to a specific genetic link. For example:
7-Repeat Polymorphism in DDR4
DDR4 is the gene encoding the dopamine D4 receptor, and has been under investigation as being related to childhood maladaptive behavior
A 2000 study (Lakatos 2000) says that a polymorphism in DDR4 is associated with disorganized attachment
But a 2018 study actually shows that this polymorphism is associated with LESS disorganized behavior (Graffi 2018)
Mutations in 5-HTTLPR region of SLC6A4 gene (gene that encodes for 5-HTT, the serotonin transporter)
5-HTT is a key regulator of serotonergic neurotransmission that affects behaviors such as food intake, reproduction, cognition and emotion (Canli 2007)
A 2007 study says that a mutation in this gene may be related to disorganized attachment
A 2016 study says there is no correlation (Brumariu 2016)
Is Disorganized Attachment Just Someone’s “Temperament?”
Temperament can be thought of as a person’s natural predisposition.
In 11k patients, one study found that “Temperament was not significantly associated with disorganized (d = .11, CI [0.03, 0.25]) attachment” (Groh 2017)
“The emergence of disorganized attachment is not related significantly to gender or temperament” (Shemmings & Shemmings 2011 p.55)
I think this is helpful because the question is whether there is a link between a difficult child and developing disorganized attachment. It was important to be able to see if children with high disagreeable traits move in the direction of disorganized attachment, and these studies show that is not the case.
I think these studies show that disorganized attachment is not due to genes or temperament (from what we can tell so far). It truly is a dyad relationship, which is why when the dyad changes later in life through a mentor or therapist, the patient can move out of disorganized attachment.
What Role Does The Caregiver Play In Causing A Child To Display Disorganized Attachment?
Maltreatment By Carers
The predisposing factor most likely to be associated with disorganized attachment is maltreatment by a carer. The abuse and neglect of a child is far more likely than any other single factor to lead to disorganized-attachment behavior because it is at the heart of what disorganized attachment means. “The paradox for the child is that the very person who should be able to protect him or her is at one the same time the source of danger” (Shemmings & Shemmings 2011, p. 54).
In the Leiden meta-analysis, the combined effect size across five studies focusing on childhood maltreatment and disorganized attachment was impressive (r= .41) (van IJzendoorn et al. 1999).
In maltreating parents (n=165), 48% of children were found to be disorganized compared to 14% in low risk groups
The percentage rose to 77% when only the Main and Solomon codings were used. A 2008 study found that “90% of maltreated infants were disorganized, compared to 43% of low income controls” (Lyons-Ruth and Jacobvitz 2008 p.668)
A 2010 meta-analysis produced large effect sizes in that maltreated children are more likely to be disorganized (effect size = 2.19) than other socioeconomically at-risk children (effect size = 0.48) (Cyr 2010).
Of these ten studies, only seven studies examined disorganized attachment. Despite this small set of studies, “our estimates of combined effect sizes reported for attachment security and disorganization of maltreated children show lower 95% confidence boundaries that are still more than 1.5 SD from zero, again pointing to large effect sizes” (Cyr 2010)
Also, because of the small set of studies, the meta-analysis was unable to statistically test for differences between physically abused and neglected children, although both types of maltreatment seem to have a similar impact on attachment
Also, childhood maltreatment and disorganized attachment in infancy are both predictors of future dissociative symptoms, so it’s interesting to note that maltreatment is associated with disorganized attachment.
It is important to note, however, that maltreatment by carers is not the only cause of disorganized attachment.
Maternal Unresolved Trauma
There is a consistent relationship between parental unresolved loss and trauma, and infant disorganized attachment. Many studies consider disorganized attachment as being a second-generation effect of trauma that had been inflicted on the disorganized infant’s parent.
A 1995 meta-analysis of 10 studies involving 548 participants demonstrated that parents who were classified as “unresolved” in the adult attachment interview showed overlap with corresponding disorganized infant attachment classification with a combined effect size of r=.31 (van IJzendoorn, 1995).
It’s important to see that this effect size is nowhere near as important as maltreatment. So, if you’re a mother who has suffered from trauma it does not mean that you are hopelessly damaging your child. If anything, a parent who has suffered trauma probably just needs encouragement. Therapy can be helpful but the effect size of .3 is not as large as someone who abuses their child.
How can parental unresolved loss lead to disorganized attachment? The parents’ behavior represents an “attempt to defend themselves against re-experiencing the fear, helplessness and anger associated with the trauma may result in repeated failure to comfort and soothe children when their attachment system is activated” (Out et al. 2009, pp.420-421).
Another suggestion of how unresolved loss may emerge later on when a survivor becomes a caregiver is “mothers with a history of physical abuse or witnessed violence were more likely to display the hostile profile of behaviour at home, while mothers with a history of sexual abuse or parental loss (but not physical abuse) were more likely to withdraw from interaction with their infants” (Lyons-Ruth 2003, p. 893).
Also, 62% of adults diagnosed with dissociative disorders had mothers who had lost a close relative within two years of their children’s birth (Dozier 2008b p. 730). So, conceivably, the adults with dissociative disorders may have had disorganized attachment patterns as infants as a consequence of maternal unresolved attachment classification.
Parents living with unresolved trauma may behave in a frightening or frightened manner toward their child during the strange situation procedure. The caregiver is often unresolved with respect to attachment, and is thus unable to protect the child adequately from later threats, and may even cause the child to feel threatened (Hesse & Main, 2006).
Examples of frightening or frightened (FR) parental behavior include:
Parent making unpredictable invasions of infant space (ie, coming up from behind infant, or moving hand across infant’s face or throat), baring teeth, unusual vocalizations, scary pursuits of baby, trance-like or dissociative states that last more than thirty seconds, and covering the baby’s face with stuffed toys. Also, stiff handling of the baby, as if the baby were an inanimate object, or suddenly retreating from the baby as if fearful of being hurt, and making guarded postures (Hazen 2014).
What does it mean if a parent displays frightening or frightened behavior?
Many parents who exhibit FR behavior are otherwise sensitive and responsive to the needs of their children. The parents exhibit FR behavior as a result of having endured major loss or maltreatment themselves. This is sometimes termed the “first-generation effect”. Thus, the disorganized attachment pattern in the child can therefore be viewed as a “second-generation effect” of the parent’s prior trauma (Hesse & Main, 2006)
Individuals with socioeconomic risk factors may be more likely to display frightened or frightening behavior and we will discuss this in a later section
Below is a table from Hesse & Main 2006 that describes unresolved/disorganized behaviors in adults. The offspring of individuals with these behaviors are at risk for disorganized attachment patterns (Hesse & Main 2006).

(Table 2 from Hesse & Main, 2006, p. 315)
Parental Withdrawal Behavior
A 2003 study suggests that levels of parental withdrawal are significantly higher in children with disorganized attachment patterns compared to children with organized attachment patterns (Goldberg 2003). Withdrawal is defined in this study as “lack of response”, and “can be as fear provoking for the child as behavior that is frightening in and of itself” (Goldberg 2003, pp. 242-43). There was no significant difference amongst disrupted parenting behaviors (such as fearful/disoriented, intrusiveness/negativity) between organized and disorganized children.
You can see the effects that a lack of response has on a child in the still face experiment. A parent with a spaced out look can be extremely distressing for the child. I see this in couples therapy as well where the husband or the wife is spacing out and then the other partner gets upset that their partner is not engaging or hearing what is being said.
According to a 2013 study, “Maternal withdrawal in infancy was a significant predictor of both borderline symptoms and suicidality/self-injury in late adolescence” (Lyons-Ruth, 2013).
Maternal withdrawal-disrupted communication at 18 months predicted BPD symptoms (Beta 0.45, p = 0.001)
Maternal Major Depressive Disorder (MDD)
According to Shemmings & Shemmings 2011 book Understanding Disorganized Attachment: Theory and Practice for Working with Children and Adults, there is minimal relationship between mothers with depressive disorders and subsequent disorganized attachment patterns in their children.
“Depressed carers, parents using drugs and alcohol to excess, carers experiencing relational disharmony; none of these adults are necessarily acting in ways toward their children to cause them harm. Witnessing domestic violence, seeing a parent desperately sad (but without knowing why) and watching a carer progressively ‘lose it’ with drink or drug are never optimal for a child’s development, but these behaviors in themselves do not necessarily lead children to lack an organized strategy to seek and maintain proximity when their attachment system is activated” (Shemmings & Shemmings 2011 p. 56).
In accordance, only 19% of children whose parents were living with depression showed disorganized attachment behaviors (van IJzendoorn et al. 1999). There were no significant differences compared to the normative 14%.
But, in contrast, other studies suggest that maternal depression may be a factor that results in disorganized behavior (see Martins 2000 and Toth 2006).
According to a 2006 study, “Mothers with MDD have been shown to be less sensitive parents, to exhibit greater negativity and less positive affect during mother–child interactions, and to be poor disciplinarians [...] Children of depressed mothers also have been shown to be at increased risk for the development of insecure attachment relationships, because they often have experienced maternal physical and psychological unavailability” (Toth 2006).
When I see depressed mothers, I know that the sooner I can effectively treat this mother the better. If the mother can get out of the depression she can make up for lost time and can create that attunement and connection with her child. I also recommend for family members of depressed mothers to come visit more, or for the husband to stay home more. It can be hard to fathom, but a significantly depressed mother really influences small children. We want to help mothers out of depression by getting them into therapy and, if necessary, prescribe medication. If they’re not out of depression within 2 months, I will highly recommend an intensive outpatient program where they can get therapy 3-5 days a week. It can be difficult to initially get a mother to go to outpatient therapy because she wants to be home with her child. But, if the depression is suicidal and she doesn’t want to be with the child, I will immediately suggest outpatient intensive care.
Helping the mother get back to a better state is crucial because we know that babies who have had depressed mothers react differently to the still face experiment. We know there is an increase in both insecure and avoidant attachment, and decreased rates of secure attachment. In some cases I’ll need to bring in the husband or partner and discuss how important it is for the mother to get treatment so that they can support her.
This paper studied three groups:
group one was mothers who had experienced MDD since their child’s birth that DID NOT participate in toddler-parent psychotherapy
group two was mothers who had experienced MDD since their child’s that DID participate in toddler-parent psychotherapy
Group three was a control group, comprising non-depressed mothers.
What they found was that both MDD groups had significantly higher rates of [infant] disorganized attachment than the [non-depressed mother control] group — 19.1%, χ2 (1, n = 133) = 5.80, p < .02 and χ2 (1, n = 132) = 7.33, p < .01, respectively (Toth 2006).
A 2000 meta-analysis of seven studies (one study was discarded because it was an outlier) of middle-income families with no risk factors other than maternal depression was conducted.
“Infants of depressed mothers showed significantly reduced likelihood of secure (B) attachment and marginally raised likelihood of avoidant (A) and disorganised (D) attachment. The first two effects varied considerably in magnitude between studies, whereas the increase in disorganised attachment, from 17 % to 28 % on average, was consistent” (Martins 2000).
Infants of depressed mothers showed:
Significantly reduced likelihood of secure (B) attachment
Weighted pooled Z =-3.827
but also much variability, because the χ2 value of 14.408 is close to significance,”
Marginally raised likelihood of avoidant (A) attachment
Weighted Z = 2.365
χ2 = 10.576 (variable)
Marginally raised likelihood of disorganised (D) attachment
Weighted Z = 2.342
χ2 =3.509 (homogenous)
Maternal Borderline Personality Disorder (BPD)
Although the Shemmings & Shemmings 2011 book Understanding Disorganized Attachment: Theory and Practice for Working with Children and Adults does not touch on maternal BPD, there are several studies that suggest it plays a role in the formation of disorganized attachment.
According to a 2005 study:
80% of 12 month olds with mothers with BPD were classified as D type, as compared to only 27% of 12-month-olds with mothers without BPD (Hobson 2005)
Medium effect size (d = .66), and the group contrast was significant, (p = .02) (Hobson 2005)
“BPD showed lower levels of ‘availability for positive engagement’, lower ratings of ‘behavior organization and mood state’, and a lower proportion of interpersonally directed looks that were positive; (b) in the Strange Situation, a higher proportion (8 out of 10) of infants of borderline mothers were categorized as Disorganized; and (c) in play, mothers with BPD were rated as more ‘intrusively insensitive’ toward their infants” (Hobson 2005)
BPD also led to infants having more disinhibited behavior to strangers compared to controls and depressed mothers (Hobson 2005)
This is another high risk group that I deeply care about. Nobody asks to have BPD, and mothers who suffer from it don’t want to hurt their children. That’s why it’s so important for these patients to get the psychotherapy and treatment that they need. It’s never too late to get treatment.
What Social Factors Are Associated With Disorganized Attachment?
Pre-pregnancy Exposure to Alcohol
Pre-pregnancy exposure to alcohol has been associated with disorganized attachment, whereas alcohol during pregnancy increases risk of insecure attachment and later suicidal behavior.
I’ve had patients adopt kids with fetal alcohol syndrome who also have been exposed to meth or fentanyl in the womb, putting them at a higher risk. (Those who adopt these kids are making a real difference in the world)
This study uses absolute alcohol (AA) score, which yields average daily ounces of alcohol consumed. For example, two drinks of wine, beer, or liquor is about 1.0 oz of absolute alcohol, and the AA score is 1.0.
In this study, the mean AA score for mothers prior to pregnancy was .80 (SD = .93) which is equivalent to 1.75 drinks per day, and during pregnancy mean AA score was .21 (SD=.30), which is equivalent to 1.33 drinks per day (O’Connor 1987)
Prior to pregnancy, mothers of secure infants had an average AA score of 1.0, or one drink per day, whereas mothers of disorganized infants had an average pre-pregnancy AA score of 1.36 (SD = 1.19), which is approximately three drinks per day (O’Connor 1987)
Marital Conflict Between Caregivers
Marital conflict might play a small role in disorganized attachment behavior (r2= .21 I = .19, FI = 8.08, p< .01, d = 1, 35) (Owen 1997)
r2= .21 is indicative of a small correlation
In this study, “marital conflict” was defined by video taping marital interactions and rating them via the Beavers-Timberlawn Family Evaluation Scale, prenatally and at 3 months
Extensive Non-Maternal Care
Infants who have extensive non-maternal care may be at increased risk for developing disorganized attachment (Hazen 2014).
Hazen 2014 examined two samples, Austin, (n = 125), and NICHD (n = 1,135) to determine whether a maximum threshold of time spent in nonmaternal care exists, beyond which infants might have an increased risk of forming disorganized infant-mother attachment patterns (Hazen 2014).
The Austin sample yielded the following information: Infants with over 60 hours per week in nonmaternal care were significantly more likely to have a disorganized attachment with their mothers, Wald x2 (1) = 4.35, p = .037 (Hazen 2014)
The NICHD sample demonstrated that the risk of disorganized attachment increases exponentially when hours of non-maternal care exceeds 60 hours per week (Hazen 2014)
If you are going to put your child in daycare, it’s important to observe what a normal day is like and to look at reviews and talk to parents who have children in that daycare to make sure they won’t be exposed to poor quality adult interactions. Most people have to spend some time away from their children because they have to work, but make sure your child is with someone who is connecting with them.
Cumulative Socio-Economic Risk Factors
As we discussed above, childhood maltreatment is the strongest predictor for disorganized attachment and is stronger than socioeconomic risk factors.
However, data from that same study also demonstrates that children with five or more socioeconomic risks (k = 8 studies, effect size = 1.20) “were not significantly less likely to be disorganized than maltreated children” (Cyr 2010).
In this study, the risk indicators were: low income, substance abuse, ethnic minority group, single parenthood, adolescent mother (<20 years), and low education (<12 years) (Cyr 2010). Socioeconomic and environmental stressors such as poverty, isolation, and racism affect parental coping, and may cause the parent to behave in a frightened or frightening manner (Cyr 2010).
This is important to keep in mind when interpreting claims that higher rates of disorganized attachment exist among children of single mothers and children of mothers of a racial and/or ethnic minority, who are more likely to be living in poverty (Cyr 2010).
Significantly more disorganized attachments were found in studies with single minority mothers in comparison with studies of single caucasian mothers (Cyr 2010)
Disorganized attachments in studies with single minority groups:
d = 0.86, k = 14, n = 1,510
“The data on ethnicity shows that most mothers of minority groups were also single” (Cyr 2010, p. 99).
"Being a single mother may limit access to financial or social resources, increase social isolation, and maternal stress, and result in inadequate caregiving behavior and child disorganized attachment” (Cyr 2010, p. 99).
Mothers working two jobs and/or the child/mother experiencing racial trauma is a big part of this factor. It’s not that the mothers are more abusive, because maltreatment is a lot higher than this effect size. At the same time, how do we build programs to support these mothers? How do we create daycares that are an enriching and supportive environment.
Raising kids is exhausting and I can’t imagine doing it alone. I don’t have all the answers right now, but it’s important for these circumstances to be on our radars. This is part of the complex racial issue that is part of the bigger issue right now. I think we can make a big difference if we pay close attention to this data. We want to utilize this information to make the world a better place. How do we decrease disorganized attachment and intergenerational trauma? Empathy goes a long way.
Disorganized attachments in studies of single Caucasian mothers
d = 0.01, k = 7, n = 789, Q = 4.43, p =.04
This study shows a higher proportion of disorganized children in families with a minority group mother in comparison to families with a caucasian mother. What could explain these differences?
“Unfortunately, we were not able to contrast single and non single mothers from minority groups because there were only two studies of minority group mothers that were not single. Being a single mother may limit access to financial or social resources, increase social isolation, and maternal stress, and result in inadequate caregiving behavior and child disorganized attachment. This process seems to be more problematic for children of high-risk minority group mothers than for those of high-risk Caucasian mothers.” “Bakermans-Kranenburg et al. 2004 demonstrated that the link between low-income African American families and child attachment insecurity which was partially mediated by maternal insensitivity, and that low income appeared to be a more important factor than ethnicity. […] Additional stressors such as the experience of racism or isolating language barriers might play an important role” (Cyr 2010, p. 104).
According to Bakermans-Kranenburg et al. 2004, there are three separate processes that result in difference in attachment security between African-American and white children.
“Attachment measures may be culturally biased and yield unwarrantedly low scores for security in cultural groups different from the culture in which the measures were developed” (Bakermans-Kranenburg et al. 2004 p. 418).
“Associations between attachment quality and assumed precursors of secure attachment may be divergent in different cultural contexts” (Bakermans-Kranenburg et al. 2004 p. 418).
“A third variable, related to ethnicity and attachment, may be responsible for differences in attachment security between the two groups” (Bakermans-Kranenburg et al. 2004 p. 418).
Having 5 socioeconomic risk factors plays a role in the development of disorganized attachment (Cyr 2010):
The set of studies with five risk indicators (low income, substance abuse, ethnic minority group, single parenthood, adolescent mother (<20 years), and low education (<12 years)), showed a significantly higher proportion of disorganized children (d = 1.20, k = 8, N = 429) in comparison with children from low-risk backgrounds
Similar differences were not found for the sets of studies with:
one to two risk indicators (d = 0.33, k = 11, N = 555)
three risk indicators (d = 20.03, k = 7, N = 606)
or four risk indicators (d = 0.54, k = 8, N =1,296).
The post hoc contrast between studies with five risks versus studies with fewer than five risks was also significant (Q = 7.12, p < .01)
“Hence, children living in families characterized by five risk indicators were significantly more likely to be disorganized than children living in families characterized by a lower number of risks” (Cyr 2010)
Next, they compared presence of disorganization between children who were maltreated and children living in families characterized by five risk indicators:
“To test whether non-maltreated children living under the impact of a high number of risks were as likely as maltreated children to show secure attachment behavior, we compared studies of maltreated children (k = 10) with studies on non-maltreated children with the highest level of risk (five risk indicators, k = 10),” (Cyr 2010).
A significant contrast was found (Q = 27.99, p = .01), showing that maltreated children (average number of risk indicators: M = 2.50, SD = 0.27) were less likely to develop secure attachment than children exposed to five risk indicators.
However, the contrast for disorganization was not significant
(Q = 2.07, p = .15)
“Hence, children living in families characterized by five risk indicators (k = 8 studies, d =1.20) did not show significantly less attachment disorganization than maltreated children” (Cyr 2010)
(k = 7 studies; average number of risk indicators: M = 2.43, SD = 0.30).
Figure 1 [see below] presents the combined effect sizes for risk indicators and maltreatment status,” (Cyr 2010).

(Figure 1 from Cyr 2010)
Are There Any Biomarkers Of Disorganized Attachment?
A biomarker is defined as “a distinct biochemical, genetic, or molecular characteristic or substance that is an indicator of a particular biological condition or process” (Dictionary.com). In this section we will discuss the following biomarkers as they relate to disorganized attachment: CRP levels, left amygdala volume, diurnal cortisol secretion patterns, and cortisol attunement between mother-infant dyads.
CRP & BMI
A study from 2018 describes association between elevated CRP (C-Reactive Protein, a marker of inflammation) levels during early childhood being associated with a history of disorganized attachment during infancy. They studied children that had histories of being involved with CPS (child protective services), and children with no CPS involvement.
They found that CPS-referred children with disorganized (or insecure) attachment during infancy had higher levels of CRP in early childhood than CPS-referred children who had secure attachment during infancy, and higher levels of CRP compared to low-risk comparison children with no history of being involved with CPS (Bernard 2018)
“CPS- referred children with insecure or disorganized attachments had significantly higher CRP levels than both low-risk children (p = 0.010) and CPS-referred children with secure attachments (p = 0.026)” (Bernard 2018)
CPS-referred children with secure attachment during infancy had similar CRP levels to low-risk comparison children with no history of being involved with CPS (Bernard 2018)
“CPS-referred children with secure attachments did not differ significantly from low-risk children (p = 0.705)” (Bernard 2018)
Below is a table showing the log-transformed CRP levels for each group in the study. As you can see, there is a much higher CRP level for children in the insecure/disorganized group, as compared to both the secure and the comparison group.

(Figure 1 from Bernard 2018)
This same study also highlights the importance of CRP in association with BMI because elevated CRP in early childhood is associated with increases in BMI over time (Bernard 2018).
In bivariate correlations, early childhood CRP was associated with BMI at age 4, r (45) = 0.26, p = .08), and BMI at age 8, r (37) = .52, p = .001)
Hierarchical multiple regression demonstrated that early childhood CRP levels significantly predicted BMI at age 8, controlling for BMI at age 4
This suggests that elevated CRP in early childhood was associated with increases in BMI over time
Increased Left Amygdala Volume
According to a 2016 study, the volume of the left amygdala can be predicted by the quality of an infant’s attachment pattern at 18 months of age. Disorganized attachment interactions result in increased left amygdala volume in adulthood, which is associated with dissociation and limbic irritability (Lyons-Ruth, 2016).
Limbic irritability refers to a variety of somatic symptoms that may stem from increased excitatory neurotransmission following childhood maltreatment (Dackis 2012)
As described earlier, dissociation is a long-term ramification of disorganized attachment behavior during infancy
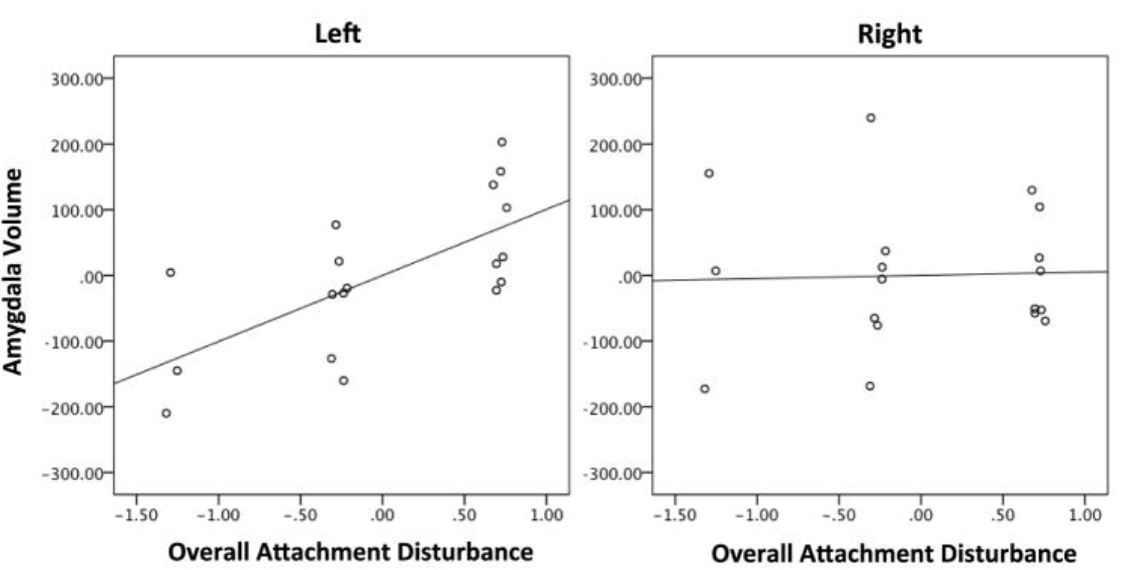
Amygdala volume was normalized and adjusted for total grey matter volume and race. Left (r = .679, p = .004) but not right (r = −.048, p = .860) amygdala volume was related to overall attachment disturbance (Lyons-Ruth, 2016).

Amygdala volume was normalized and adjusted for total grey matter volume and race. Left amygdala volume was strongly related to both limbic irritability (r = .770, p = .001) and dissociative symptoms (r = .586, p = .017) in adulthood, controlling for total grey matter volume and race (Lyons-Ruth, 2016).
Respiratory Sinus Arrhythmia
The autonomic nervous system regulates our physiological responses to stress. This is referring to the “fight or flight” phenomenon. For example, if you were to unexpectedly stumble upon a tiger, your autonomic nervous system would be responsible for elevating your heart rate, dilating your pupils, redirecting blood flow away from your digestive system, and so on. So in theory, disorganized infants who are exposed to stressful situations (e.g. frightening maternal behavior) may have unique autonomic responses that are not seen in children with other attachment styles.
One way to quantitatively study a person’s autonomic nervous system is to utilize what is called respiratory sinus arrhythmia, or RSA. RSA is the physiological fluctuations in a person’s heart rate during inhalation and exhalation. Normally, a person’s heart rate increases during inhalation and decreases during exhalation (Grossman & Taylor 2007, p. 263). If someone is in a calm, connected state, they have a good RSA.
RSA is considered to be a measure of someone’s vagal tone, or the activity of the vagus nerve, which is a major regulator of the parasympathetic branch of the autonomic nervous system (Grossman & Taylor 2007, p. 263). Vagal tone (as measured by RSA) has implications over a person’s central nervous system, so RSA has been associated with emotional responding and behavior regulation (Beauchaine 2001).
Conceivably, if a person has atypical autonomic nervous system regulation patterns (such as a person who was classified as having disorganized attachment patterns during infancy), the RSA could be a quantitative measurement that might reflect disorganized attachment. The RSA is interesting because it fits into what it means to be in a more dissociated state or fight and flight state. A lot of therapy that we give to borderline personality disorder patients is mindfulness, yoga, and regulating their nervous system through calm breathing. You can learn more about RSA in my polyvagal episode.
These two studies further suggest that RSA patterns can be linked to disorganized attachment:
The first study (Tharner 2013) suggests that disorganized infants of depressed mothers have a lower resting RSA
The second study (Holochwost 2014) suggests that disorganized infants have a higher reactive RSA
The first study suggests that infants who are both disorganized and have mothers who are living with depression have a lower resting RSA as compared to children with just one of these risk factors (either disorganization or maternal depression) (Tharner 2013).
This study included 450 mother-infant dyads (disorganized infants: n = 94, 20.9%, and non disorganized infants: n = 356), and the mean age of the infant was 14 months (M = 14.7, SD = 0.9)
Dyads were observed in a modified strange situation procedure (SSP) to measure attachment patterns, and maternal depression was measured 2 months postpartum using the Brief Symptom Inventory (BSI) depression scale
There was no direct association of infant-mother attachment with autonomic functioning. (see table 2 below)
There was also no direct association of maternal depressive symptoms with infant autonomic functioning (see table 2 below)
However, the study found a significant interaction effect of a combination of both maternal depressive symptoms and infant attachment disorganization on infant resting RSA:
B = 0.37,SE = 0.16, p = .02, mean R2 = .01
“Post hoc analyses revealed that higher levels of maternal postnatal depressive symptoms were associated with lower resting RSA in disorganized infants but not in non-disorganized infants” (Tharner 2013).
The same study also investigated whether disorganized infants were vulnerable to the effects of maternal depressive symptoms.
In the group of disorganized infants, higher levels of maternal depressive symptoms were associated with lower infant resting RSA:
B = -0.31, SE = 0.15, p = .04, mean R2 =.05
Whereas in non-disorganized infants, maternal depressive symptoms were not associated with infant RSA:
B = 0.05, SE = 0.06, p = .36” (Tharner 2013)

(Table 2 from Tharner 2013)
The second study suggests that disorganized infants demonstrate a higher reactive RSA, meaning elevated RSA during a stressful interaction (Holochwost 2014). It also shows that these infants are not in a rest and relaxation place naturally. They are more in the fight/flight or dissociative state. When they’re stressed, their RSA goes up even higher to compensate for the stress response, or possibly because their situation is more stressful.
This study consisted of mother infant dyads (n = 95), who were seen at ages 6 months and 12 months.
At the 6 month visit:
Baseline cardiac data were collected and parenting behaviors were assessed
Dyads participated in the Still Face Paradigm (SFP)
RSA of the infant was measured during the SFP encounter
At the 12 month visit, the children participated in the Strange Situation Procedure (SSP), in order to categorize infant attachment patterns
This study demonstrated that infants with elevated RSA during interactive (stressful) periods of the SSP at 6 months showed more attachment disorganization during the SSP at 12 months, but only if their mothers showed negative and intrusive interactions (Holochwost 2014).
“Post hoc probing of the interactions between negative-intrusiveness and RSA during normal interaction and reunion episodes revealed parallel patterns of results” (Holochwost 2014 p. 1426)
“As is suggested by Figure 1 (see below), during normal interaction and at low levels of RSA (-1 SD = 2.58), the slope defining the relationship between negative- intrusiveness and disorganization is not significantly different from zero (p = .598)” (Holochwost 2014 p. 1426)
“However, when RSA is high (+1 SD = 4.58), a positive relationship between negative-intrusiveness and disorganization is observed (B = 1.15, SE = .321; t = 3.58, p <.001)” (Holochwost 2014 p. 1426)
“Similarly, during the reunion episode no relationship is observed between negative-intrusiveness and disorganization at low levels of RSA (p = .632) but at high levels of RSA a positive relationship is observed (B = 1.09, SE = .535, t = 2.04, p = .045)” (Holochwost 2014 p. 1426)

(Figure 1 from Holochwost 2014)
To summarize, RSA values may potentially function as a biomarker for future disorganized attachment behavior, however there are still other factors that overlap (such as maternal depression, and maternal negative and intrusive interactions) that render RSA and disorganization an area for further research.
Atypical Cortisol Secretion Patterns
Typically, there is a diurnal pattern of production of glucocorticoids (e.g. cortisol) produced by the hypothalamic-pituitary-adrenal cortex (HPA) system, which involves a morning peak and an evening nadir. This diurnal pattern is established by 12 weeks of age (Price, Close & Fielding, 1983).
A look at atypical cortisol secretion in children in foster care:
A 2006 study demonstrated that children in foster care have different rates of change in cortisol over the day as compared to non-foster care controls (Dozier 2006).
Participants were between the ages of 20 and 60 months (M=32.7, SD=9.3), N=159.
Of the 159 children:
55 were children who had been placed in foster care as infants
104 comparison children who had continuously lived with their parents.
Caregivers were to collect saliva samples from the children three times a day during a 2 day period (when the child woke up, at 2pm or prior to a nap, and at bedtime).
The study found that foster children had lower levels of “wake-up” cortisol compared to controls.
Wake-up cortisol values were significantly higher for comparison children than for foster children (Dozier 2006, p. 193).
F(1,140) = 8.43, p< .01
Differences were not significant for afternoon or bedtime levels, but the difference between wakeup and bedtime values was greater for comparison children than for foster children (Dozier 2006, p. 193).
F(1, 140)= 5.22, p< .05
Both groups’ cortisol levels decreased throughout the day, but differed in how much they decreased from morning to evening (Dozier 2006, p. 193).
Comparison group: F(1,95) = 178.24, p < .01
Foster care group: F(2,42) = 61.12, p < .01

(Figure 1 from Dozier 2006)
Atypical cortisol secretion in children with disorganized-attachment pattern:
Four years after the above study was published, another study described a “flattened” diurnal cortisol pattern in disorganized children when compared to non-disorganized children (Luijk 2010).
The children in this study were roughly 14 months of age, with 40 classified as disorganized, and 138 classified as non-disorganized
A limitation of this study is that there are significantly more subjects classified as non-disorganized than organized
Upon observing cortisol excretion throughout the day, a main effect of disorganization was found for slope
(F (1, 213) = 3.99, p < .01, n2 = .03) (Luijk 2010, p. 447)
Disorganized children have a flatter slope in daily cortisol secretion than non-disorganized children
Disorganized slope = -.84, SE = .11
Non-disorganized slope = -1.16, SE = .06 (Luijk 2010, p. 447)

(Figure 3 from Luijk 2010, p. 447)
Calculating an individual’s slope of cortisol diurnal rhythm might be a useful marker for identifying individuals who would benefit from specific therapeutic interventions that target disorganized-attachment behavioral patterns.
What Therapies Work For Treating Children And Families Experiencing Disorganized Attachment?
Attachment and Biobehavioral Catch-up (ABC)
ABC was specifically designed to help a child improve attachment organization (Bernard 2012). It consists of 10 sessions, each with specific goals:
Sessions 1-2: Parents learn to provide nurturance when the child is distressed by re-interpreting the child’s alienating behavior
Sessions 3-4: Parents provide a sensitive, responsive environment by following the child’s lead with delight when child not distressed
Sessions 5-6: Parents learn to behave in ways that are not frightening to child
Sessions 7-8: Parents learn to provide nurturance when child is distressed by overriding their own issues that interfere with providing nurturing care
Sessions 9-10: Parents learn the importance of touch and young children’s emotions (Bernard 2012)
A 2012 randomized clinical trial reports “children in the ABC intervention showed significantly lower rates of disorganized attachment (32%) and higher rates of secure attachment (52%) relative to control intervention (57% and 33% respectively)” (Bernard 2012).
Participants included 120 children and 113 parents (7 parents had two children enrolled in the study)
Participants were identified by agencies working with child protective services in a large, mid-Atlantic city. All parents had been enrolled in a program that assists in diverting children from foster care and remaining with biological parents. They had been enrolled in this program due to identified needs or concerns (including domestic violence, parental substance abuse, homelessness and child neglect)
Of the children enrolled in the study, 60 were randomly assigned to receive ABC intervention, and 60 were randomly assigned to receive Developmental Education for Families (DEF) as the control.
Children and parents participated in videotaped SSP before and after intervention, and attachment patterns were classified by two coders
Results:
Children in the ABC intervention group showed lower rates of disorganized attachment as compared to the DEF control group
χ2 (1,120) = 7.60, p< .01, Medium effect size (d = 0.52)
Following intervention, 32% of ABC children had disorganized attachment, whereas 57% of DEF children had disorganized attachment.
Children in the ABC intervention group showed significantly higher rates of secure attachment, relative to the DEF control group
χ2 (1,120) = 4.13, p < .05, medium effect size (d = 0.38)
Following intervention, 52% of ABC children had secure attachment, versus 33% of DEF children having secure attachment
Results did not remain significant when excluding children who were older than 24 months at the time of the second SSP
χ2 (1,95) = 1.85, p > .05
Small effect size (d=0.28)
Results remained significant when excluding the second child of the seven parents who had two children in the study
χ2 (1,113)=4.85, p < .05
Medium effect size (d=0.44)
In terms of biomarkers, a study published in 2008 found that following ABC therapy, disorganized children in foster care demonstrated more typical patterns of cortisol secretion and that this pattern did not differ significantly from the control group (non-foster care children) (Dozier et al. 2008b).
According to a study published in 2019, ABC may also be an effective strategy to prevent disorganized attachment behaviors.
This study explored the utility of ABC in modifying “disrupted parenting behavior”, (including affective communication errors, role/boundary confusion, fearful/disoriented, intrusive/negativity and withdrawal) in association with child disorganized attachment. The study demonstrated that “parents who received ABC demonstrated lower levels of parental withdrawal than parents who received the control condition [...] Results add to the efficacy of the ABC intervention and identified parental withdrawal as a mediator of change” (Yarger 2019).
As mentioned earlier, parental withdrawal behavior is a contributor to child’s disorganized attachment. Withdrawal in this study is defined as “lack of response”, and “can be as fear provoking for the child as behavior that is frightening in and of itself” (Goldberg 2003, pp. 242-43).
A significant effect of intervention on parental withdrawal was revealed (F(1, 104)=4.59, p=.03), such that:
Parents who received ABC demonstrated significantly lower levels of withdrawal (M=3.76, SD=1.44) compared to parents who received DEF (control) (M=4.42, SD=1.69)
Small to medium effect size (Cohen’s d = -0.42) (Yarger 2019)
ABC seems to have positive effects on biological and behavioral outcomes, and is likely a useful intervention for children living with disorganized attachment patterns. It may also be a useful preventative method by way of decreasing parental withdrawal behaviors.
Group Attachment-Based Intervention (GABI)
GABI is a trauma-informed approach with the primary goal of promoting secure parent-child attachment, and possibly preventing the late sequelae that infants with disorganized-attachment may experience, such as social isolation.
GABI also focuses on trauma experienced by parents, which, as stated earlier, may result in frightening or withdrawal behavior towards the child, possibly resulting in disorganized-attachment behavior in the child.
In GABI, parents and children (birth to 3 years old) are seen 3 times per week for two hours. GABI functions as a “group therapy” and has many benefits supporting parents and children living with disorganized-attachment patterns, such as:
It allows parents to support each other. Parents of children with disorganized attachment behavior often are living with unresolved trauma. (GABI is a setting in which parents with similar backgrounds and responses can interact with and learn from one another)
GABI facilitates social interactions between children with disorganized attachment patterns, who otherwise might have been subject to peer isolation and social rejection (Murphy 2015)
At the time of writing, there is no research surrounding whether GABI diminishes and/or prevents disorganized-attachment patterns, although a 2019 trial demonstrated GABI as being superior to current standard parenting classes in terms of improving parent-child relationships, as evidenced by higher levels of “dyadic reciprocity.”
Dyadic reciprocity is defined as a healthy synchronous relationship between infant and childhood and is linked to healthy adaptation and well-regulated psychological and physiological functioning (Feldman 2007)
The study involved 78 families with “children less than 3 years old and their mothers who were regarded at risk of maltreating their children by referral agencies” (Steele 2019, p. 203)
“Mothers’ risk status derived from a heavy trauma burden (average exposure over the first 18 years of their lives to 10 possible adverse childhood experiences [ACEs] was >5), mental health challenges (15-28% had experienced a prior psychiatric hospitalization), and prior removal of a child to foster care (20%)” (Steele 2019, p. 203)
Mothers were randomly assigned to the parenting class, Systemic Training for Effective Parenting (STEP), or GABI
“The adjusted end-of-treatment means [...] reveal[s] that children and mothers who participated in GABI showed 0.88 higher levels of dyadic reciprocity than children and mothers who participated in STEP (GABI = 3.29, STEP = 2.41, with the covariate in the model dyadic reciprocity at baseline being evaluated at 2.51). In other words, children and mothers in GABI showed significantly more dyadic reciprocity as compared to intake in contrast to children and their mothers in STEP, who showed slightly lower levels of dyadic reciprocity than shown at intake” (Steele 2019, p. 211)
This study does not specifically comment on modification of disorganized attachment; “We await the completion of reliable masked scoring of the Strange Situation assessments, including 6-month follow up data that will yield a more definitive account of the extent to which GABI improves the quality of the child-mother relationship and in particular, if attachment disorganization can be diminished by GABI” (Steele 2019 p. 215). Future studies must be performed to assess the utility of GABI in improving disorganized-attachment behaviors.
Transference Focused Psychotherapy (TFP)
TFP is an intervention that targets individuals living with borderline personality disorder, and a 2006 randomized control trial (Levy 2006) describes how it may be used to change attachment patterns from unresolved/disorganized to secure.
TFP is carried out in 2-3 face-to-face sessions per week where the patient carries out free association as the therapist assists them in identifying difficulty in reflecting on his or her own behavior and interactions (Kernberg 2008).
The general indication for TFP is for patients with borderline personality organization. This includes individuals who present with:
Severe identity diffusion, defined as: the “incapacity to accurately assess self and others in depth, to commit in depth to work or a profession, to establish and maintain intimate relationships, and in a lack of the normal subtlety of understanding and tact in interpersonal situations” (Kernberg 2008)
Severe breakdown in work, intimate relationships, and in social life
These symptoms are generally thought of as features of BPD and other cluster B personality disorders. However, these behaviors may also be present in adults who displayed disorganized-attachment behaviors earlier in life, but do not otherwise fit the full criteria for BPD.
With that in mind, TFP might be a useful intervention for adults who are classified as “unresolved/disorganized” on the Adult Attachment Interview (AAI), as this classification is considered to be a direct equivalent of disorganized attachment patterns during the SSP in infancy.
To recap, this is what classifies a person as “unresolved/disorganized” on the AAI:
The person displays “lapses in the monitoring of reasoning or discourse when discussing experiences of loss and abuse. These lapses include highly implausible statements regarding the causes and consequences of traumatic attachment-related events, loss of memory for attachment-related traumas, and confusion and silence around discussion of trauma or loss” (Levy 2006)
This is the “adult form” of disorganized attachment
Contrast with “secure attachment” on the AAI:
A “Secure/Autonomous Individual” will present a well-organized, coherent description of early attachment relationships, and freely express emotions and discuss concrete examples when discussing both positive and negative early relationships. They view attachment based relationships as being very influential to their own personal development (Levy 2006)
According to Levy 2006, an individual’s attachment style may actually become “secure” following TFP.
The study’s participants were individuals living with BPD and were assigned to TFP, Dialectical Behavior Therapy (DBT) and supportive psychotherapy (SPT). AAI was conducted before and after the intervention, and changes in attachment patterns were documented.
In the Transference Focused Therapy group, at time 1 (pre-treatment), 1 of 22 individuals (4.5%) were classified as having a secure attachment. However, after treatment, 7 out of 22 patients were classified as having a secure attachment (χ2 (1, N =22) =4.17, p <.04)
There was no change, however, for DBT or SPT in the number of patients who went from insecure to secure attachment. The difference in the number of securely attached patients between the TFP and DBT and SPT cells was obviously not significant at Time 1, with (χ2 (2, N=60) = 1.46, p >.05), but was significant at the end of treatment (χ2 (2, N=60) = 8.25, p < .02)
The study also showed how TFT had more improvements in reflective function and attachment coherence.
In summary, this study describes how TFP is a more effective therapeutic intervention for individuals with disorganized attachment patterns compared to DBT and/or supportive psychotherapy.
Video-Feedback Intervention to Promote Positive Parenting and Sensitive Discipline (VIPP-SD)
VIPP-SD is “an intervention aimed at enhancing sensitivity and firm limit-setting in parents, and reducing behavior problems in children” (Juffer 2018).
A 2017 meta-analysis (figure 2) of 12 randomized control trials (N = 1116 parents and caregivers) found that “VIPP-SD proved to be effective in promoting sensitive caregiving, while positive social-emotional child outcomes were also found” (Juffer 2017).
Combined effect size for improved child outcomes (d = 0.37, k = 8, N = 721)
The 12 studies included:
At-risk children (adopted children, children at risk of externalizing problem behavior, children with autism, infants at risk of autism)
Parents at risk or in special situations (Parents classified as insecure on the AAI, parents with eating disorders, insensitive parents, maltreating parents, ethnic-minority parents, and highly-deprived, high-risk parents in a poverty context)

(Figure 2 from Juffer 2017)
Let’s look at a study that focuses on VIPP-SD specifically in the context of children with disorganized attachment.
A 2011 randomized control trial evaluates “the efficacy of a short-term attachment-based intervention for changing risk outcomes for children of maltreating families was examined using a randomized control trial. Sixty-seven primary caregivers reported for maltreatment and their children (1–5 years) were randomly assigned to an intervention or control group” (Moss 2011).
Intervention Group: 8 weekly home visits directed at caregiver-child dyad and focused on improving caregiver sensitivity. Intervention sessions included discussions about attachment-emotion regulation-related themes and video feedback of parent-child interaction” (Moss 2011)
“To perform these analyses, four attachment change groups (from pretest to posttest) were computed for organization/disorganization (organized to organized, organized to disorganized, disorganized to disorganized, and disorganized to organized)” (Moss 2011, p. 204).
The chi-square analysis was significant (See Table 7 below):
χ² (3, N = 67) = 10.91, p < .05 (effect size: r = .37) (Moss 2011, p. 205)
“Post hoc analyses revealed that a greater proportion of disorganized children in the intervention group became organized (37.1%, z = 2.00) in comparison with the control group (15.6%, z = -2.00)” (Moss 2011, p. 205)
Also, only one child in the intervention group became disorganized (2.9%, z = 22.40) in comparison with seven in the control group (21.9%, z = 2.40) (Moss 2011, p. 205)

(Table 7 from Moss 2011, p. 205)
In summary, video feedback seems to be an effective intervention in helping parents and children struggling with disorganized attachment behaviors.
Strategies To Prevent Disorganized Attachment
Secure Attachment Family Education (SAFE)
SAFE promotes secure infant-parent attachment and to prevent the transmission of unresolved trauma from parents to their infants. SAFE begins during pregnancy (targeting parents living with unresolved trauma) and consists of group and individual sessions, and continues until the infants’ first birthday (Walter 2019).
SAFE consists of four basic elements to promote secure infant-parent attachment:
Enhancement of parental sensitivity in infant-parent interaction using video-based sensitivity training prenatally, and individual video feedback postnatally
Reflection on parents’ own early and later attachment experiences and unresolved trauma
Psychoeducation about attachment theory and general knowledge of child development
Provision of social support by the facilitator and the group of other parents (Walter 2019)
A recent 2019 study revealed that there was no difference in disorganized attachment between the SAFE group and the control group in terms of attachment behaviors between infant and mother. However, the results suggest that SAFE is beneficial in terms of enhancing secure attachment between infants and their fathers (Walter 2019).
Infant-father attachment:
In the SAFE group, post-intervention, 84.6% of infants showed a secure attachment relationship with their fathers, whereas 65.8% of the infants in the control group were coded as securely attached
The difference in the distribution of attachment security in fathers was statistically significant (χ2 [1,77] = 3.67, p = .049, Cramer’s V = .22)
Regarding attachment disorganization, no group differences were found (χ2 [1,77] = 0.14, p = .481, Cramer’s V = .04) (Walter 2019)
Infant-Mother Attachment:
In the SAFE group, post-intervention, 66.7% of the infants were securely attached to their mothers, whereas in the control group 64.0% of the infants were securely attached to their mothers
The difference in the distribution of attachment security in the two conditions was not statistically significant (χ2 [1,104] = 0.08, p = .468, Cramer’s V = .03, odds ratio = 1.13)
In the SAFE group 85.2% and in the control group 88.0% of the infants showed an organized pattern of attachment to their mother
The difference is not significant (χ2 [1,104] = 0.18, p = .449, Cramer’s V = .04, odds ratio = 0.78) (Walter 2019)
According to this study, the lack of significant effects on infant-mother attachment “may conceivably be a cause of the others’ greater psychological stress compared to the fathers’ lower levels. [...] Furthermore, 18.8% of the mothers but no father (sic) reported having participated because they felt vulnerable due to their own attachment experiences” (Walter 2019, p. 17).
“Babywearing”
“Babywearing is a term often used in Western culture to describe the practice of holding or carrying an infant in a soft cloth carrier (e.g. slings, soft-structured carrier with buckles, woven or stretchy wraps, Asian-inspired traditional carriers) while engaging in day-to-day activities” (Williams 2020).
A new 2020 study describes hours spent infant carrying, or “babywearing,” may be an effective way to protect against development of disorganized attachment.
Adolescent mothers (Mage=19.1 years, SD = 2.0; 40.6% Hispanic; 40% < = 11th grade) were randomly assigned to one of two groups:
An infant-carrying condition at 2–4 weeks postpartum (n = 16; 1 hour/day for 3 months)
Control group (n = 17; reading a book to their babies)
The hypothesis was that the infant-carrying group would be more likely to have securely-attached infants at 7 months (M = 29.0 weeks, SD = 3.4).
The study found that hours spent babywearing is negatively correlated with disorganized attachment (rpb =−0.36) and positively correlated with secure attachment (rpb = .40) (Williams 2020). “The results suggest that infant carrying may be an effective tool at promoting secure attachments, particularly for mothers and infants at greater risk for attachment insecurity” (Williams 2020).
Toddler-Parent Psychotherapy (TTP)
As discussed previously in this document, maternal MDD may lead to disorganized attachment behavior, so could therapy that focuses on MDD in mothers prevent disorganized-attachment behaviors?
One 2006 study suggests that TTP may be effective in fostering secure-attachment relationships in children of mothers with MDD. “Mothers who had experienced MDD since their child’s birth were recruited (n = 130) and randomized to toddler–parent psychotherapy (DI), or to a control group (DC). Nondepressed mothers (with no current or history of major mental disorder) and their toddlers (averaging 20.34 months of age at the initial assessment) were recruited for a nondepressed comparison group (NC; n = 68). Higher rates of insecure attachment were present in both the DI and the DC groups at baseline, relative to the NC group.
Post intervention, at 36 months old, insecure attachment continued to predominate in the DC group. In contrast, the rate of secure attachment had increased substantially in the DI group and was higher than that of the DC and the NC groups. These results demonstrate the efficacy of toddler–parent psychotherapy in fostering secure-attachment relationships in young children of depressed mothers” (Toth 2006).
In Summary
I want to re-emphasize the power of empathy and the power of connection. If someone does have disorganized attachment, connection over time will be part of the solution. We really can help and there are plenty of therapeutic offerings for every age if they are dealing with the difficulties of having a disorganized attachment style. It can be difficult with this population because internal states are not as transparent, which is why microexpression training, empathy training, and therapeutic alliance can make a huge impact for these patients.