
Episode 236: Clozapine & Schizophrenia with Michael Cummings, MD
Date Published: 3/28/25
Liam Browning, Joanie Burns, DNP, APRN, PMHNP-BC, Al-Baab Khan, David Puder, MD
Corresponding author: David Puder, MD
Peer reviewed: Erika Vega, MD
By listening to this episode, you can earn 1.75 Psychiatry CME Credits.
Other Places to listen: iTunes, Spotify
Clozapine remains the gold-standard antipsychotic for treatment-resistant schizophrenia (TRS). Discovered in the 1950s and reintroduced in 1989 after initial concerns about agranulocytosis (Khokhar et al., 2018), clozapine has a unique efficacy in patients who fail to respond to other antipsychotics. It is also the only FDA-approved agent to reduce suicidal behavior in schizophrenia and schizoaffective disorder, and this advantage translates into lower overall mortality. Despite its unparalleled benefits, clozapine is underutilized due to its complex side effect profile and monitoring requirements (Dell’Osso et al., 2024). This article provides an up-to-date clinical guide on clozapine for practicing psychiatrists, synthesizing current research, and insights from an interview with Dr. Michael Cummings. We will review clozapine’s pharmacology, best practices for initiation and side effect management, and emerging uses.
The FDA is Ending Clozapine REMS
On February 25th, 2025, the FDA rescinded the Risk Evaluation and Mitigation Strategy (REMS) for clozapine. Clozapine had been pulled from the market in the 1970s after fatal cases of severe neutropenia in Finland, but the pivotal Kane and colleagues trial in 1988 showed clozapine to be highly effective for treatment-resistant schizophrenia. In order to bring the drug back to the market, the REMS imposed stringent requirements on clinicians and patients.
Under REMS, prescribers were required to monitor absolute neutrophil counts (ANC) weekly for the first six months, then every two weeks for another six months, and monthly thereafter (Dell’Osso et al., 2024). The cumulative 12-month risk of any neutropenia (ANC < 1500/μ) is about 3-4%, while severe, life-threatening neutropenia (ANC < 500/μ) is about 0.8-0.9% (Li et al., 2020; Myles et al, 2018). However, data show that the absolute risk of severe neutropenia peaks during the first three months, then drops to roughly 1 in 6,000–10,000 after the one-year mark—a rate comparable to other non-chemotherapy drugs that can affect the bone marrow (e.g., anticonvulsants, antibiotics, antithyroid medications, fluoxetine, etc.).

Note. Reprinted from “Clozapine-induced agranulocytosis. Incidence and risk factors in the United States”, by Alvir et al., 1993, New England Journal of Medicine, 329, 162–167.
To ensure proper oversight following these risk patterns, many European guidelines have required only weekly monitoring for 18 weeks, then monthly until one year, and discontinued routine checks thereafter. Morbidity and mortality rates in Europe are on par with those seen under the stricter U.S. REMS, indicating that the REMS schedule for monitoring does not significantly improve safety—but presents a barrier to using the medication.
With the REMS program abolished, the FDA no longer imposes a centralized or mandatory monitoring schedule for clozapine, shifting the responsibility to clinicians. They advise clinicians to follow best practices as outlined in the prescribing information and use clinical judgment, especially in the high-risk window of the first 6 months:
Weekly ANC checks for the first 6 months.
Every 2 weeks for the next 6 months.
Option to discontinue mandatory routine checks after 12 months, provided the patient has had no episodes of significant neutropenia, remains clinically stable, and is properly educated on early signs of infection.
The advent of rapid, point-of-care fingerstick ANC testing also offers an additional practical advantage, as it simplifies lab checks and further reduces barriers. With these changes, more patients will have access to this life-changing medication.
Indications and Unique Efficacy in Schizophrenia
Clozapine’s primary indication is treatment-resistant schizophrenia, defined by failure to respond to at least two antipsychotic trials that were of adequate duration (6 or more weeks) and dose (therapeutic plasma levels or an LAI). Approximately one-third of people with schizophrenia meet this criterion. Once these criteria are met, the odds of a patient achieving remission with a non-clozapine antipsychotic are less than 7% (Howes et al., 2017), compared to about 40% with clozapine. In one study response rate was 53.2% in the optimal range of 223–558 ng/mL (Northwood et al., 2023). However, if treatment-resistant schizophrenia is not addressed early on, Clozapine’s effectiveness begins to decline (40%-60% to around 30%). Therefore, it is beneficial to switch patients sooner to offer the best chance for improvement.
In addition to symptom reduction, clozapine is the only FDA-approved drug to reduce recurrent suicidal behavior in schizophrenia or schizoaffective disorder (Dell’Osso et al., 2024). This stems from the InterSePT trial findings that patients treated with clozapine (n = 490) showed less suicidal behavior compared to patients treated with olanzapine (n = 490; 20.8% vs. 28.8%, 26% relative risk reduction) (Meltzer et al., 2003).
Clozapine is also effective for comorbid aggression and violence. Research and clinical consensus indicate that clozapine can reduce hostile and aggressive behaviors in schizophrenia more than other antipsychotics and that this may be independent of its effects on psychotic symptoms or sedation, but can be attributed to its effects on cognition and executive functioning (Faden & Citrome, 2024).
Emerging and Off-Label Uses: Beyond schizophrenia, clozapine’s off-label uses are expanding. Low-dose clozapine is highly effective for Parkinson’s disease psychosis, treating hallucinations without exacerbating motor symptoms (Friedman, 2022). It was the first antipsychotic shown to improve Parkinson’s psychosis while improving tremor in some cases (Taylor et al., 2022). However, because Parkinson’s patients are prone to aspiration and clozapine can increase saliva production, it is important to weigh these risks and benefits appropriately (see below section on managing side effects). Clozapine has also been used in treatment-refractory bipolar disorder (especially with psychotic features or rapid cycling), though evidence is primarily from case series. Additionally, emerging research supports clozapine’s efficacy in catatonia, particularly when associated with schizophrenia or treatment-resistant psychotic disorders (Saini et al., 2024). “An important caveat with catatonia is catatonia is always a secondary syndrome…so you ultimately have to treat the underlying condition if you hope to control catatonia,” Dr. Cummings states. Clozapine may not only treat underlying psychosis but also modulate GABAergic and glutamatergic pathways implicated in catatonia. It has shown promise in benzodiazepine-refractory cases and, in some instances, may reduce reliance on electroconvulsive therapy (ECT) for chronic catatonic states.
Pharmacology: Mechanism of Action and Receptor Profile
Clozapine’s efficacy and side effect profile are best understood through its distinctive pharmacology. It is classified as a “multi-receptor” atypical antipsychotic, with a mechanism markedly different from first-generation antipsychotics (FGAs):
Dopamine Receptor Binding: Clozapine is a relatively weak dopamine D₂ receptor antagonist, with fast dissociation kinetics and less than 20-68% D₂ receptor occupancy at therapeutic doses (Nordström et al., 1995). This contrasts with FGAs and the -dones subclass of antipsychotics (e.g. risperidone), which require ~70–80% D₂ blockade for antipsychotic effect and often exceed the threshold for extrapyramidal symptoms (EPS) (de Greef et al., 2011). Clozapine’s lower striatal D₂ occupancy, especially in the nigrostriatal pathway, explains its minimal EPS liability (de Greef et al., 2011). Its inverse agonist activity on 5-HT2A has also been proposed to increase nigrostriatal dopamine release while decreasing mesolimbic dopamine, thereby treating psychosis without causing significant parkinsonism (Dell’Osso et al., 2024). Interestingly, clozapine does bind D₄ receptors with high affinity, though the clinical significance of D₄ blockade is unclear.
Serotonin Antagonism: Clozapine potently acts as an antagonist at 5-HT2A receptors (more specifically, it is an inverse agonist at 5-HT2A, as it decreases 5-HT2A activity when bound, unlike true antagonists that simply prevent agonist binding without changing receptor activity) (Li et al., 2014). By blocking 5-HT2A in the cortex and striatum, clozapine disinhibits dopamine release in the striatum, counteracting D₂ blockade effects on movement (Dell’Osso et al., 2024). This mechanism, in addition to its limited dopamine antagonism at therapeutic doses, explains why clozapine has lower risks of EPS compared to other antipsychotics. 5-HT2A antagonism may also contribute to improvements in negative symptoms and mood.
Adrenergic, Muscarinic, and Histaminergic Effects: Clozapine’s broad receptor profile includes antagonism at α₂-adrenergic receptors, multiple muscarinic acetylcholine receptors, and H₁ and H₂ histamine receptors (Dell’Osso et al., 2024):
α₂-Adrenergic antagonism may enhance norepinephrine and dopamine release in the prefrontal cortex, which some hypothesize helps with negative symptoms and cognitive deficits (Dell’Osso et al., 2024).
α₁-adrenergic antagonism contributes to orthostatic hypotension.
Muscarinic receptor antagonist (M1–M5), particularly at M1, M3, and M5. Dr. Cummings notes that 50-100 mg of clozapine is as anticholinergic as 1 mg of benztropine (de Leon, 2005). This underlies many side effects (e.g. constipation, tachycardia, urinary retention, blurred vision). When high doses of clozapine are stopped abruptly, this can lead to a rebound cholinergic delirium due to the greater number of M receptors available to bind to acetylcholine (Stanilla et al.,1997). This rebound can also be associated with other classic symptoms of excessive cholinergic activity, such as sweating, nausea, diarrhea, urinary urgency, insomnia, and vivid dreams. If stopping clozapine abruptly due to serious complications such as severe neutropenia or myocarditis, start benztropine (or another strong anticholinergic [e.g. trihexyphenidyl, diphenhydramine]) at the equivalent dose (1 mg benztropine per 50-100 mg clozapine). Otherwise, taper clozapine gradually to reduce the likelihood of cholinergic rebound and EPS if initiating an antipsychotic with strong D2 antagonism.
Norclozapine, the active metabolite of clozapine, is also thought to act as a muscarinic partial agonist on M4 receptors of salivary glands, contributing to drooling.
Histamine H₁ blockade explains the prominent sedation and weight gain, while H2 interactions have been speculated to aid clozapine’s efficacy in TRS (Dell’Osso et al., 2024).
Key point: Do not stop clozapine abruptly! Sudden withdrawal could cause delirium…
Pharmacokinetics: Smoking and Drug-Drug Interactions with Clozapine
After oral administration, clozapine’s plasma half-life typically ranges from about 8 to 16 hours (though it can be longer in chronic use or at higher doses), and the parent drug is extensively transformed by CYP1A2 and, to a lesser extent, by CYP3A4 and CYP2D6 into the active metabolite N-desmethylclozapine (norclozapine) and clozapine N-oxide, an inactive metabolite.
Smoking can dramatically affect clozapine levels. The aryl hydrocarbons produced by cigarette smoking (not the nicotine) induces CYP1A2, leading to a significant decrease in plasma levels. As little as 7-12 cigarettes per day can induce CYP1A2 activity, and full induction of the enzyme increases its activity by about 1.7 fold (Haslemo et al., 2006; Zhou et al., 2009). Therefore, smokers often require 50% higher doses, and if a patient stops smoking, clozapine levels can rise sharply, risking toxicity. Routine inquiry about tobacco use (including cannabis smoking) is essential, as is coordinating any smoking cessation with proactive dose adjustment (Blacker, 2020; Montville et al., 2021). Other drugs, such as phenytoin, rifampin, and carbamazepine can induce CYP3A4.
Nicotine vaping (e.g., e-cigs, vapes), however, do not affect clozapine levels like cigarettes do. Therefore if a patient switches from cigarette smoking to vaping, plasma concentrations of clozapine can increase drastically, so similar precautions must take place.
Key point: consistent smoking or caffeine habits should be maintained once a clozapine dose is established, or doses must be adjusted with changes.
Drugs with the greatest inhibitory effect on CYP1A2 include fluvoxamine, ciprofloxacin, and enoxacin can increase clozapine levels by 2- to 5-fold. Similarly, high amounts of caffeine (in excess of 400mg) can mildly raise clozapine levels (about 5-10%) by competing for CYP1A2 (Hägg et al., 2000).
Here are tables summarizing how various CYP450 enzyme inducers, inhibitors, and other factors impact clozapine levels and metabolism (see alsoEpisode 141):


Initiation and Dosing Strategies for Clozapine
Initiating clozapine requires a gradual titration to balance efficacy, tolerability, and safety. The standard approach is to “start low and go slow.”
A typical schedule begins at 12.5-25 mg once at bedtime on day 1. Giving the initial doses at bedtime is recommended because clozapine’s sedative and orthostatic effects (via α₁ and H1 receptors) are most prominent when initiating the drug. If this dose it tolerated, then increase to 12.5-25 mg twice daily, then up to 100mg per day by the end of the first week and 200mg per day by the end of the second week.
Slower titration of 50 mg increments (or less) once or twice per week is recommended to allow the body to acclimate to clozapine’s sedative and cardiovascular effects and reduces the risk of seizures. It usually takes about 2–3 weeks to reach a therapeutic dose (e.g. 300+ mg/day), though titration can be faster in a hospital setting with close monitoring. Dr. Cummings notes that after a dose increase it takes only about two weeks to reach 80% of that dose’s expected plasma concentration, so titrating slower than two week increments is unnecessary in most cases.
Therapeutic Dosing and Monitoring Plasma Concentrations
The effective dose range for clozapine in schizophrenia is broad (usually 200–600 mg/day). Many patients respond around 300–450 mg/day, but some require higher doses (600–900 mg/day) for full remission. Importantly, response is correlated with plasma clozapine levels.
Therapeutic drug monitoring is recommended to ensure plasma levels are above approximately 350 ng/mL, which is often cited as the minimum level for response, according to a recent meta-analysis (Northwood et al., 2023). Plasma concentrations can be expected to scale nearly 1:1 with oral dosing in men (350 mg dose = 350 ng/mL plasma level), while plasma concentrations in women scale at about 1:1.3 (350mg dose = about 500 ng/mL plasma level). Dr. Cummings mentions that with dosing, pushing higher concentrations can lead the patient to develop intolerable side effects or saturate the utility of the drug.
When patients are not responding as expected, monitoring plasma concentrations can distinguish between a pharmacokinetic issue (“pseudo-resistance” due to rapid metabolism) that leads to subtherapeutic plasma levels versus true clozapine resistance. For example, a non-smoking patient on 400 mg nightly with a plasma level of only 200 ng/mL may be an ultra-rapid metabolizer or non-adherent, whereas a patient with plasma levels of 500 ng/mL and no response after 3 months may require even higher plasma levels as tolerated (Dr. Cummings notes plasma concentrations may need to be titrated up to 1000 ng/mL and even up to 1400 ng/mL in very rare cases, but this is off-label, and done in a controlled setting with high monitoring and expertise) or further augmentation strategies such as ECT or adding a second antipsychotic (e.g. aripiprazole).
Augmentation and Combination
For patients who are truly clozapine-resistant, confirmed by ensuring adequate plasma levels for 8 to 12 weeks and ruling out pharmacokinetic interactions, several augmentation strategies may be considered.
Addition of a Second Antipsychotic:
Although evidence supporting this strategy is limited, (Chiu et al., 2020), Tiihonen and colleagues (2019) conducted a large cohort study following over 62,000 patients for 20 years and found that patients treated with a combination of clozapine and aripiprazole had a 14% lower risk of psychiatric hospitalization compared to those on clozapine monotherapy, and that this combination was associated with the lowest hospitalization rates among all tested. However, combinations of clozapine with other antipsychotics did not significantly reduce hospitalization rates compared to clozapine alone.
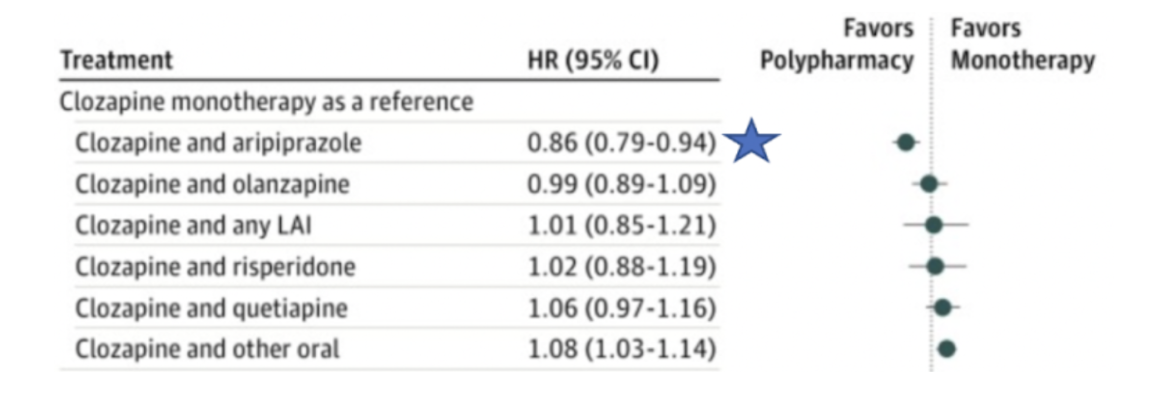
Note. Reprinted from “Association of Antipsychotic Polypharmacy vs Monotherapy With Psychiatric Rehospitalization Among Adults With Schizophrenia”, by Tiihonen et al., 2019, JAMA psychiatry, 76(5), 499–507.
When combining another antipsychotic with clozapine, it is important to choose an agent that has a complementary binding profile to clozapine. For example, clozapine’s antimuscarinic effects block the action of xanomeline, whereas antipsychotics acting on D2 receptors (such as aripiprazole) are more appropriate.
ECT augmentation
A meta-analysis by Wang et al. (2018) examined 18 RCTs, primarily conducted in China, and found that patients receiving ECT augmentation showed greater symptom improvement (effect size 1.4) and remission rates compared to those on clozapine alone. However, a more recent sham-controlled trial by Melzer-Ribeiro et al. (2024) found no significant differences in symptoms or remission rates after 20 ECT sessions. Nevertheless, ECT may be particularly useful in those with catatonic or affective features (Grover et al., 2023).
Antipsychotic Polypharmacy Without Clozapine:
For patients who are not candidates for clozapine due to intolerance or logistical barriers, combining two non-clozapine antipsychotics can be considered. Dr. Cummings notes that the goal with polypharmacy is to combine different mechanisms of action hoping for additive benefits in treatment (see also Episode 214). According to the Tiihonen et al. (2019) meta-analysis, selecting antipsychotics with complementary receptor binding profiles is a rational approach. For example, a high-affinity D2 antagonist such as haloperidol could be paired with a second-generation antipsychotic with broader receptor activity, such as olanzapine. This outcome is still inferior to clozapine’s efficacy and will expose the patient to a greater risk of EPS if both agents are used at high doses (Carnahan et al., 2006; Taipale et al., 2023).

Note. Reprinted from “Association of Antipsychotic Polypharmacy vs Monotherapy With Psychiatric Rehospitalization Among Adults With Schizophrenia”, by Tiihonen et al., 2019, JAMA psychiatry, 76(5), 499–507.

Note. Reprinted from “Association of Antipsychotic Polypharmacy vs Monotherapy With Psychiatric Rehospitalization Among Adults With Schizophrenia”, by Tiihonen et al., 2019, JAMA psychiatry, 76(5), 499–507.
Monitoring and Managing Side Effects
Clozapine’s side effect profile is extensive, spanning nearly every organ system. Up to 40% of patients discontinue clozapine within 2 years due to side effects or non-adherence (Dell’Osso et al., 2024; Lieberman & Stroup, 2011). However, most side effects are manageable with vigilant monitoring and targeted interventions, and despite the increased risk of severe side effects compared to other antipsychotics, all-cause mortality is lower in patients treated with clozapine (Hayes et al., 2015).
Hematologic: Neutropenia
As discussed above, the most notorious clozapine complication is severe neutropenia, or agranulocytosis. Clozapine-induced agranulocytosis occurs in roughly 0.5-1% of patients, typically within the first six months of treatment (Myles et al., 2018). Due to mandatory blood count monitoring through REMS, the fatality rate of clozapine agranulocytosis has fallen to around 2.7–3% (much lower than the ~7–10% mortality for agranulocytosis from other causes) (Dell’Osso et al., 2024). The overall death rate from agranulocytosis in patients exposed to clozapine is less than 0.05% (Myles et al., 2018).
Known risk factors for clozapine induced neutropenia include concurrent valproate use, older age, female sex, and Asian ethnicity, as well as certain HLA genetic polymorphisms (HLA-DQB1 6672G>C [rs113332494], HLA-B38:01) (Legge et al., 2019; Konte et al., 2021). However, it should be noted that the genetics underlying clozapine-induced neutropenia are likely multifactorial and that having these genetic variants does not preclude initiation of the drug.
Management of Neutropenia: If neutropenia occurs, management depends on severity.
Mild neutropenia (ANC 1000–1500/µL): Increase monitoring frequency to three times weekly until ANC reaches above 1500/µL.
Moderate neutropenia (ANC 500-999/µL): Stop clozapine treatment until ANC normalizes. ANC should be checked daily until it returns to above 1000/µL, then three times weekly until ANC reaches above 1500/µL, and then weekly for an additional 4 weeks. After ANC stabilizes, a rechallenge can be initiated. A hematology consult is recommended.
Severe neutropenia (agranulocytosis, ANC < 500/µL): Stop clozapine, consult hematology, and initiate infection precautions. ANC checks should proceed following the same protocol as moderate neutropenia (daily until above 1000/µL then 3x/week until above 1500/µL). A rechallenge is not recommended unless the prescriber determines the risks of treatment outweigh the benefits.
Augmenting Neutrophil Count Granulocyte Colony-Stimulating Factor (G-CSF, or filgrastim) can accelerate neutrophil recovery for a clozapine rechallenge. A 2023 systematic review found that clozapine rechallenge with G-CSF support can be effective regardless of initial agranulocytosis severity (Corbeil et al., 2023). In addition to G-CSF, lithium can also be used to induce granulocytosis via enhancing production of G-CSF and stimulating proliferation of pluripotent stem cells (Focosi et al., 2009).
Benign ethnic neutropenia is a genetic variant in individuals of African or Middle Eastern descent that periodically lowers baseline ANC (<1500/µL) without a concomitant increased risk of infection. Guidelines allow adjusted ANC thresholds in such cases so that clozapine is not inappropriately withheld. If suspected in a patient, consult hematology to establish the diagnosis by ruling out other potential causes and to pursue genetic testing.
Cardiovascular: Myocarditis, Cardiomyopathy, and Hypotension
Serious cardiac side effects of clozapine, though rare, have garnered increased attention. Myocarditis, a potentially fatal complication, occurs in an estimated 0.02–1.2% of clozapine patients and is thought to be the result of a hypersensitivity reaction. Notably, about 50% of cases present within the first month of treatment (median onset ~2–3 weeks) and rarely occur thereafter (Bellissima et al., 2018). Vital signs (heart rate, temperature), labs (troponins and CRP), and symptoms (chest pain, fatigue) should be monitored at each weekly visit during the first 6 weeks (Segev et al., 2021). Some experts recommend a baseline echocardiogram as well.
The most common presentation is an unexplained fever with associated chest pain or malaise. However, benign fever is a common complaint, occurring in up to 20% of patients initiated on clozapine. If a patient does have a fever during the first 8 weeks, best practice is to send the patient to the ED for a workup that includes a physical exam, CBC, troponins, CRP, and imaging, if needed. If myocarditis is confirmed (e.g. via markedly elevated troponin or echocardiogram findings), clozapine must be stopped and cardiology consulted. There is no notable consensus on rechallenge after myocarditis; it has been done successfully in select cases after recovery, but only with extreme caution and perhaps a very slow titration (Manu et al., 2018).
Cardiomyopathy (dilated heart failure from long-term toxicity) is another rare complication (estimated <5% incidence), and unlike other complications of clozapine, it typically occurs after months or years of treatment. It should be suspected if a patient develops insidious dyspnea, edema, or exercise intolerance. Annual physical exams (and possibly periodic echocardiograms in high-risk individuals) are prudent to catch late cardiomyopathy. As with myocarditis, cardiomyopathy usually necessitates stopping clozapine (Murch et al., 2013).
On the benign end of the spectrum, sinus tachycardia is very common with clozapine, seen in up to 25% of patients (Dell’Osso et al., 2024). Clozapine’s anticholinergic and adrenergic effects increase heart rate. This resting tachycardia often peaks during titration and may subside over 4–6 weeks. Unless the heart rate is >120 or symptomatic, it can be monitored; if persistent, a low-dose beta blocker (e.g. atenolol 25–50 mg) can be used after the initial titration period (Dell’Osso et al., 2024). (Beta blockers should be avoided in the first 6 weeks unless absolutely needed, as they could mask early signs of myocarditis). Educating the patient about hydration and avoiding caffeine (which can worsen tachycardia) is also helpful, and determining whether the tachycardia is secondary to orthostasis is crucial.
Orthostatic hypotension frequently occurs during the first two weeks of titration due to α₁ blockade and sedation. Patients should be warned to rise slowly and stay hydrated. Most will develop tolerance by week 4. If significant dizziness or near-syncope occurs, the titration speed should be slowed or held. In severe cases, addition of midodrine or fludrocortisone can support blood pressure (Dell’Osso et al., 2024), but these are rarely needed if titration is cautious. Hypertension on clozapine is uncommon, but if it emerges later in treatment, it may relate to weight gain and metabolic changes; standard antihypertensives can be used as needed (Dell’Osso et al., 2024).
Neurologic: Seizures, Sedation, and Neuropsychiatric Effects of Clozapine
Seizures: Clozapine lowers the seizure threshold in a dose-dependent manner. At doses <300 mg the risk is low (<1%), but at higher doses (600–900 mg) the risk of generalized seizures rises to around 3–5% (Dell’Osso et al., 2024). Myoclonic jerks can precede generalized seizures in some patients. Electroencephalogram (EEG) abnormalities, including generalized slowing and epileptiform discharges, are also prevalent among clozapine-treated patients, occurring in approximately 50% to 60% of cases (Hatano et al., 2023). To mitigate this risk, slow titration and using the lowest effective dose are essential (Dell’Osso et al., 2024).
If a patient has a seizure on clozapine, first ensure their clozapine level is not supra-therapeutic or rising too quickly. Typically, you would temporarily halt clozapine or reduce the dose, then add an anticonvulsant. Once stabilized, clozapine can be cautiously resumed at a lower dose alongside the anticonvulsant. “...Seizure, per se, is not a reason to stop clozapine…It’s a reason to add an antiepileptic to prevent the seizures,” says Dr. Cummings. Prophylactic valproate or lamotrigine can be considered in patients with epilepsy or EEG abnormalities before starting clozapine, or those needing very high clozapine doses (Varma et al., 2011). However, valproate can also lead to neutropenia in a dose-dependent manner and is also teratogenic in both men and women.
Sedation: Nearly all patients experience sedation on clozapine, especially during initiation. Histamine H₁ antagonism and anticholinergic effects cause drowsiness, which is often most pronounced in the first few weeks. Sedation can be dose-limiting, but concentrating the dose at night can help minimize daytime sedation. Over time, many patients develop partial tolerance to the sedative effect as H₁ receptors adapt (Dell’Osso et al., 2024). Importantly, clozapine’s sedative and sialorrhea effects make aspiration a concern at night, especially in elderly patients and those with Parkinson’s disease.
Delirium and Miscellaneous CNS effects: Clozapine’s anticholinergic properties occasionally cause a delirium, especially at higher doses, in susceptible patients (e.g. those with baseline cognitive impairment), or when abruptly stopped due to cholinergic rebound.
Rarely, clozapine can precipitate obsessive-compulsive symptoms or worsen pre-existing OCD, likely due to clozapine’s antagonism at 5-HT2A/C receptors (Moreno Tarazona et al., 2025). Management involves lowering the clozapine dose if feasible, adding an SSRI (avoid fluvoxamine or fluoxetine), or augmenting with another antipsychotic such as aripiprazole (Kim et al., 2019). If a patient does not present entirely with schizophrenia, but has a schizoaffective disorder or bipolar disorder, the option for an antidepressant while on clozapine becomes risky.
Extrapyramidal symptoms are distinctly uncommon, but clozapine can occasionally cause tremors or rigidity (often treatable by beta-blockers or anticholinergics) and very rarely neuroleptic malignant syndrome (NMS). Interestingly, if a patient has a history of NMS to another antipsychotic, about 79% will also get NMS if re-challenged with clozapine (Dell’Osso et al., 2024), so extreme caution is warranted in such scenarios. Some evidence suggests concomitant valproate might predispose to NMS with clozapine (Dell’Osso et al., 2024).
Metabolic and Endocrine: Weight Gain, Diabetes, and Lipid Abnormalities
Clozapine is the most metabolically problematic antipsychotic. Studies report that one-third to one-half of patients on clozapine gain more than 7% of their baseline body weight, driven by H₁ histamine and 5-HT2C antagonism, which increase appetite, along with increased insulin resistance and reduced activity due to sedation. Weight gain typically starts within the first six months and can progress over time to metabolic syndrome, characterized by T2DM, hyperlipidemia, and hypercholesterolemia. Up to 26% of clozapine-treated patients develop new-onset diabetes over six years, with severe cases leading to hyperosmolar coma or diabetic ketoacidosis (McGrath et al., 2022). Baseline assessment of weight, waist circumference, blood pressure, fasting glucose and HbA1c, and lipids, then follow-up at 3 months and at least annually (more frequently if changes occur) can prevent and ameliorate cardiovascular consequences (Dell’Osso et al., 2024). Managing clozapine induced metabolic syndrome requires a proactive approach, including nutritional counseling, regular exercise, and pharmacotherapy, including metformin, GLP-1 agonists, insulin and statins (see also Episode 223.)
Managing Sialorrhea
Sialorrhea (Excessive Salivation): Paradoxically, clozapine often causes drooling (especially at night), despite having anticholinergic properties, which may be attributable to norclozapine’s partial agonist activity at M4 receptors. Up to 30–80% of patients experience sialorrhea to some degree. Dr. Cummings notes, “In many patients, that actually increases the risk of aspiration and aspiration of pneumonia. It’s one of the dangerous side effects of clozapine.”
Non-pharmacological approaches include sleeping on an incline and placing a towel over the pillow. Pharmacologically, sublingual anticholinergic drops (atropine 1% ophthalmic drops, 1–2 drops under the tongue at bedtime) often help reduce nocturnal drooling. Systemic agents like glycopyrrolate (which does not cross blood-brain barrier significantly), 1–2 mg at bedtime is a common approach that can reduce drooling with less risk of central anticholinergic side effects. Alternatively, low-dose clonidine or benztropine at night may provide some relief. Recent evidence suggests that agents from the benzamide class (such as amisulpride or metoclopramide) might also alleviate clozapine-associated sialorrhea, though this is a newer strategy and not yet widely adopted. In refractory cases, Botox injections into salivary glands have been tried. Notably, sialorrhea tends to improve over time as tolerance develops, but many patients require ongoing bedtime medication to fully control it.
Managing Constipation and Urinary Retention
Constipation and GI Hypomotility: Clozapine’s anticholinergic potency and 5-HT antagonism makes constipation the most fatal complication attributed to clozapine, as it can lead to bowel obstruction and ensuing perforation, strangulation, compartment syndrome, and sepsis (Patel et al., 2021). Importantly, hypomotility can occur regardless of treatment duration and is quite common, with some studies finding up to 30–60% of clozapine patients experience significant constipation and up to 80% experience colonic hypomotility, defined as colonic transit time greater than two standard deviations above the population mean (Every-Palmer et al., 2016). Therefore, collecting a history of baseline bowel functioning (frequency and consistency of bowel movements), performing an abdominal exam (can supplement with an abdominal X-ray), and tapering off other anticholinergic medications should be completed prior to initiating clozapine. Proactive prophylaxis is also critical: a bowel regimen with daily osmotic laxatives (polyethylene glycol) and/or stool softeners should be started at the first sign of constipation, or even preemptively in those with a history of slow bowels. Although evidence from RCTs is limited (Every-Palmer et al., 2017), many clinicians will schedule laxatives (e.g. PEG 3350 17g daily or docusate 100-250 mg QHS) for all clozapine patients to prevent severe constipation. If a patient experiences constipation and 2 days pass without bowel movement, intensify laxatives (add senna, bisacodyl if not already using, and increase docusate to max dose of 250 mg or to 125 mg BID) and monitor closely. If the patient is still constipated, perform a digital rectal exam to assess whether stool is impacted and consult GI to see if an enema or disimpaction is needed. If impacted, stop stimulant laxatives. If not impacted, consider using an intestinal secretagogue such as lubiprostone or prucalopride.
Oftentime, patients will be reluctant to use laxatives for their constipation or to disclose their symptoms, but it is important to educate patients that unlike typical constipation, this is a medication effect that must be managed daily. Clozapine-induced ileus is a medical emergency with a fatality rate of 15-28% (Cohen, 2017). If a patient on clozapine develops new abdominal pain and distension, or vomiting, an urgent evaluation (physical exam, abdominal X-ray or CT) is warranted.
Urinary retention or incontinence: Clozapine’s anticholinergic effects can also cause urinary hesitancy or retention, particularly in older men with prostate hypertrophy. If urinary retention occurs, dose reduction and urology consult (for catheterization or bethanechol, a cholinergic agent) may be needed. On the other hand, some patients experience nocturnal enuresis (bedwetting) on clozapine, possibly related to deep sedation and pelvic muscle relaxation. For enuresis, behavioral strategies (limiting evening fluids, setting an alarm to toilet at night) are first-line. If needed, desmopressin at bedtime or low-dose ephedrine/midodrine have been used in case reports to reduce enuresis (Tanzer et al., 2023).
Thromboembolism: Emerging evidence from case studies links clozapine to increased risk of venous thromboembolism (Pallares Vela et al., 2021). However, this effect may not be unique to clozapine, as sedentary behavior from sedation and weight gain are risk factors common to other antipsychotics. Clinicians should encourage mobility, manage weight, and have a high index of suspicion for symptoms like unilateral leg swelling or acute shortness of breath.
Managing Illness on Clozapine
Patients who develop severe infections can present with increased clozapine levels. Although not caused by the drug itself, cytokines interleukin 6 and interleukin 8 that are produced during severe infections can inhibit the cytochrome enzymes. During periods of illness, clozapine dose distribution should be managed carefully.
Conclusion
Clozapine is a uniquely effective antipsychotic that offers hope for patients with the most challenging forms of schizophrenia and related disorders. Its use requires a high level of clinical diligence – from slow, careful titration and blood monitoring to the anticipation and management of numerous side effects. For the practicing psychiatrist, becoming adept with clozapine greatly expands the therapeutic toolkit for treatment-resistant illness. Key takeaways include:
Unmatched Efficacy: Clozapine remains the only evidence-based option for true treatment-resistant schizophrenia, with proven advantages in reducing psychosis, preventing suicide (Dell’Osso et al., 2024), and improving life outcomes in patients who have failed other treatments. No combination of other antipsychotics has been shown to equal clozapine’s effectiveness in this population (Puder, 2024a).
Complex Pharmacology: Understanding clozapine’s receptor profile (low D₂ occupancy, high 5-HT₂A antagonism, plus noradrenergic, cholinergic, and histaminergic actions) helps predict its clinical effects – minimal EPS but prominent sedation, metabolic changes, and unique benefits in conditions like catatonia (Dell’Osso et al., 2024).
Monitoring and Side Effect Management: A structured monitoring schedule for blood counts, metabolic metrics, and cardiac symptoms is essential. Proactive side effect management (e.g. bowel regimen, exercise/diet counseling, beta blockers for tachycardia, sugar monitoring) allows most patients to remain on clozapine long-term. Severe complications like agranulocytosis and myocarditis are rare and can be mitigated by close observation during high-risk periods (Dell’Osso et al., 2024).
Special Clinical Situations: Clozapine shows efficacy beyond psychosis, notably in mitigating catatonia (alone or with ECT) (Dell’Osso et al., 2024) and in improving tardive movement disorders and akathisia (Spivak et al., 1997). It should be considered in persistent catatonia associated with schizophrenia, and tapered carefully to avoid withdrawal catatonia (Rogers et al., 2023). Its low EPS profile makes it ideal for patients intolerant of other antipsychotics due to motor side effects.
Emerging Uses: Ongoing research is exploring clozapine’s neurobiological impacts such as neurotrophic effects, and its potential benefits in mood disorders, personality disorders, and neurodevelopmental disorders. While these uses are off-label, they underscore clozapine’s far-reaching influence on the brain and behavior.
In treating severe psychiatric illness, clozapine often turns the tide for individuals who have suffered years of treatment failures. By combining vigilance in monitoring with an up-to-date knowledge of side effect management and adjunctive strategies, clinicians can use clozapine safely and effectively. The conversational insights of experienced clinicians like Dr. Cummings, backed by contemporary research, reinforce that clozapine therapy is both an art and a science – one that pays dividends in restored lives when done carefully. With systematic practice and patient education, psychiatrists can incorporate clozapine into clinical care as an authoritative yet compassionate treatment approach, offering patients with refractory schizophrenia a chance at remission and improved quality of life.
Additional episodes discussing clozapine
References:
Alvir, J. M., Lieberman, J. A., Safferman, A. Z., Schwimmer, J. L., & Schaaf, J. A. (1993). Clozapine-induced agranulocytosis. Incidence and risk factors in the United States. The New England journal of medicine, 329(3), 162–167. https://doi.org/10.1056/NEJM199307153290303
Bellissima, B. L., Tingle, M. D., Cicović, A., Alawami, M., & Kenedi, C. (2018). A systematic review of clozapine-induced myocarditis. International Journal of Cardiology, 259, 122–129. https://doi.org/10.1016/j.ijcard.2017.12.102
Blacker C. J. (2020). Clinical Issues to Consider for Clozapine Patients Who Vape: A Case Illustration. Focus (American Psychiatric Publishing), 18(1), 55–57. https://doi.org/10.1176/appi.focus.20190025
Carnahan, R. M., Lund, B. C., Perry, P. J., & Chrischilles, E. A. (2006). Increased risk of extrapyramidal side-effect treatment associated with atypical antipsychotic polytherapy. Acta psychiatrica Scandinavica, 113(2), 135–141. https://doi.org/10.1111/j.1600-0447.2005.00589.x
Chiu, Y. H., Hsu, C. Y., Lu, M. L., & Chen, C. H. (2020). Augmentation Strategies for Clozapine-Resistant Patients with Schizophrenia. Current pharmaceutical design, 26(2), 218–227. https://doi.org/10.2174/1381612826666200110102254
Cohen, D. (2017). Clozapine and Gastrointestinal Hypomotility. CNS Drugs, 31, 1083–1091. https://doi.org/10.1007/s40263-017-0481-5
Corbeil, O., Béchard, L., Fournier, É., Plante, M., Thivierge, M.-A., Lafrenière, C.-É., Huot-Lavoie, M., Brodeur, S., Essiambre, A.-M., Roy, M.-A., & Demers, M.-F. (2023). Clozapine rechallenge or continuation despite neutropenia or agranulocytosis using colony-stimulating factor: A systematic review. Journal of Psychopharmacology, 37(4), 370–377. https://doi.org/10.1177/02698811231154111
de Greef, R., Maloney, A., Olsson-Gisleskog, P., Schoemaker, J., & Panagides, J. (2011). Dopamine D2 occupancy as a biomarker for antipsychotics: quantifying the relationship with efficacy and extrapyramidal symptoms. The AAPS journal, 13(1), 121–130. https://doi.org/10.1208/s12248-010-9247-4
de Leon, J. (2005). Benztropine equivalents for antimuscarinic medication. American Journal of Psychiatry, 162(3), 627. https://doi.org/10.1176/appi.ajp.162.3.627
Dell’Osso, L., Bonelli, C., Nardi, B., Giovannoni, F., Pronestì, C., Cremone, I. M., Amatori, G., Pini, S., & Carpita, B. (2024). Rethinking Clozapine: Lights and Shadows of a Revolutionary Drug. Brain Sciences, 14(1), 103. https://doi.org/10.3390/brainsci14010103
Every-Palmer, S., Ellis, P. M., Nowitz, M., Stanley, J., Grant, E., Huthwaite, M., & Dunn, H. (2017). The Porirua Protocol in the treatment of clozapine-induced gastrointestinal hypomotility and constipation: A pre- and post-treatment study. CNS Drugs, 31, 75–85. https://doi.org/10.1007/s40263-016-0391-y
Every-Palmer, S., Nowitz, M., Stanley, J., Grant, E., Huthwaite, M., Dunn, H., & Ellis, P. M. (2016). Clozapine-treated Patients Have Marked Gastrointestinal Hypomotility, the Probable Basis of Life-threatening Gastrointestinal Complications: A Cross Sectional Study. EBioMedicine, 5, 125–134. https://doi.org/10.1016/j.ebiom.2016.02.020
Faden, J., & Citrome, L. (2024). A systematic review of clozapine for aggression and violence in patients with schizophrenia or schizoaffective disorder. Schizophrenia Research, 268, 265–281. https://doi.org/10.1016/j.schres.2023.11.008
Focosi, D., Azzarà, A., Kast, R. E., Carulli, G., & Petrini, M. (2009). Lithium and hematology: Established and proposed uses. Journal of Leukocyte Biology, 85(1), 20–28. https://doi.org/10.1189/jlb.0608388
Friedman, J.H. (2022), Clozapine Is Severely Underused in Parkinson's Disease Patients. Mov Disord Clin Pract, 9: 1021-1024. https://doi.org/10.1002/mdc3.13582
Grover, S., Sarkar, S., & Sahoo, S. (2023). Augmentation strategies for clozapine resistance: a systematic review and meta-analysis. Acta Neuropsychiatrica, 35(2), 65–75. DOI: https://doi.org/10.1017/neu.2022.30
Hägg, S., Spigset, O., Mjörndal, T., & Dahlqvist, R. (2000). Effect of caffeine on clozapine pharmacokinetics in healthy volunteers. British Journal of Clinical Pharmacology, 49(1), 59–63. https://doi.org/10.1046/j.1365-2125.2000.00111.x
Haslemo, T., Eikeseth, P. H., Tanum, L., Molden, E., & Refsum, H. (2006). The effect of variable cigarette consumption on the interaction with clozapine and olanzapine. European Journal of Clinical Pharmacology, 62(12), 1049–1053. https://doi.org/10.1007/s00228-006-0209-9
Hatano, M., Yamada, K., Matsuzaki, H., Yokoi, R., Saito, T., & Yamada, S. (2023). Analysis of clozapine-induced seizures using the Japanese Adverse Drug Event Report database. PLoS ONE, 18(6), e0287122. https://doi.org/10.1371/journal.pone.0287122
Hayes, R. D., Downs, J., Chang, C. K., Jackson, R. G., Shetty, H., Broadbent, M., Hotopf, M., & Stewart, R. (2015). The effect of clozapine on premature mortality: an assessment of clinical monitoring and other potential confounders. Schizophrenia bulletin, 41(3), 644–655. https://doi.org/10.1093/schbul/sbu120
Howes, O. D., McCutcheon, R., Agid, O., de Bartolomeis, A., van Beveren, N. J., Birnbaum, M. L., Bloomfield, M. A., Bressan, R. A., Buchanan, R. W., Carpenter, W. T., Castle, D. J., Citrome, L., Daskalakis, Z. J., Davidson, M., Drake, R. J., Dursun, S., Ebdrup, B. H., Elkis, H., Falkai, P., Fleischhacker, W. W., … Correll, C. U. (2017). Treatment-resistant schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group consensus guidelines on diagnosis and terminology. The American Journal of Psychiatry, 174(3), 216–229. https://doi.org/10.1176/appi.ajp.2016.16050503
Kane, J., Honigfeld, G., Singer, J., & Meltzer, H. (1988). Clozapine for the treatment-resistant schizophrenic: A double-blind comparison with chlorpromazine. Archives of General Psychiatry, 45(9), 789–796. https://doi.org/10.1001/archpsyc.1988.01800330013001
Khokhar, J. Y., Henricks, A. M., Sullivan, E. D. K., & Green, A. I. (2018). Unique Effects of Clozapine: A Pharmacological Perspective. Advances in pharmacology (San Diego, Calif.), 82, 137–162. https://doi.org/10.1016/bs.apha.2017.09.009
Kim, D. D., Barr, A. M., White, R. F., Honer, W. G., & Procyshyn, R. M. (2019). Clozapine-induced obsessive–compulsive symptoms: mechanisms and treatment. Journal of psychiatry & neuroscience : JPN, 44(1), 71–72. https://doi.org/10.1503/jpn.180087
Konte, B., Walters, J. T. R., Rujescu, D., Legge, S. E., Pardiñas, A. F., Cohen, D., Pirmohamed, M., Tiihonen, J., Hartmann, A. M., Bogers, J. P., van der Weide, J., van der Weide, K., Putkonen, A., Repo-Tiihonen, E., Hallikainen, T., Silva, E., Ingimarsson, O., Sigurdsson, E., Kennedy, J. L., Sullivan, P. F., … Giegling, I. (2021). HLA-DQB1 6672G>C (rs113332494) is associated with clozapine-induced neutropenia and agranulocytosis in individuals of European ancestry. Translational psychiatry, 11(1), 214. https://doi.org/10.1038/s41398-021-01322-w
Legge, S. E., & Walters, J. T. (2019). Genetics of clozapine-associated neutropenia: recent advances, challenges and future perspective. Pharmacogenomics, 20(4), 279–290. https://doi.org/10.2217/pgs-2018-0188
Li, C. H., Stratford, R. E., Velez de Mendizabal, N., Cremers, T. I. F. H., Pollock, B. G., Mulsant, B. H., Remington, G., & Bies, R. R. (2014). Prediction of brain clozapine and norclozapine concentrations in humans from a scaled pharmacokinetic model for rat brain and plasma pharmacokinetics. Journal of Translational Medicine, 12, 203. https://doi.org/10.1186/1479-5876-12-203
Li, X.-H., Zhong, X.-M., Lu, L., Zheng, W., Wang, S.-B., Rao, W.-W., Wang, S., Ng, C. H., Ungvari, G. S., Wang, G., & Xiang, Y.-T. (2020). The prevalence of agranulocytosis and related death in clozapine-treated patients: A comprehensive meta-analysis of observational studies. Psychological Medicine, 50(4), 583–594. https://doi.org/10.1017/S0033291719000369
Lieberman, J. A., & Stroup, T. S. (2011). The NIMH-CATIE schizophrenia study: What did we learn? American Journal of Psychiatry, 168(8). https://doi.org/10.1176/appi.ajp.2011.11010039
Manu, P., Lapitskaya, Y., Shaikh, A., & Nielsen, J. (2018). Clozapine rechallenge after major adverse effects: Clinical guidelines based on 259 cases. American Journal of Therapeutics, 25(2), e218–e223. https://doi.org/10.1097/MJT.0000000000000715
McGrath, N. M., Humberstone, V., & Abraham, A. C. (2022). Diabetes mellitus prevalence in Northland New Zealand schizophrenia patients on clozapine. New Zealand Medical Journal, 135(1558), 41–45. https://nzmj.org.nz/media/pages/journal/vol-135-no-1558/8572fa6ef3-1696471165/vol-135-no-1558.pdf#page=41
Meltzer, H. Y., Alphs, L., Green, A. I., Altamura, A. C., Anand, R., Bertoldi, A., Bourgeois, M., Chouinard, G., Islam, M. Z., Kane, J., Krishnan, R., Lindenmayer, J.-P., & Potkin, S. (2003). Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Archives of General Psychiatry, 60(1), 82–91. https://doi.org/10.1001/archpsyc.60.1.82
Melzer-Ribeiro, D. L., Napolitano, I. C., Leite, S. A., Alencar de Souza, J. A., Vizzotto, A. D. B., Di Sarno, E. S., Fortes, M., Gomes, M. L., de Oliveira, G. M., Avrichir, B. S., Talib, L. L., Correll, C. U., & Elkis, H. (2024). Randomized, double-blind, sham-controlled trial to evaluate the efficacy and tolerability of electroconvulsive therapy in patients with clozapine-resistant schizophrenia. Schizophrenia Research, 268, 252–260. https://doi.org/10.1016/j.schres.2023.11.009
Montville, D. J., Lindsey, J. M., & Leung, J. G. (2021). Fluctuation between cigarette smoking and use of electronic nicotine delivery systems: Impact on clozapine concentrations and clinical effect. Mental Health Clinician, 11(6), 365-368. https://www.doi.org/10.9740/mhc.2021.11.365
Moreno Tarazona, E., Orozco Gonzalez, M., La Rosa Giron, A., Ruiz-Grosso, P., & Lazo-Porras, M. (2025). Prevalence of obsessive-compulsive symptoms in patients with schizophrenia treated with clozapine: A scoping review. BMC Psychiatry, 25, 71. https://doi.org/10.1186/s12888-024-06466-9
Murch, S., Tran, N., Liew, D., Petrakis, M., Prior, D., & Castle, D. (2013). Echocardiographic monitoring for clozapine cardiac toxicity: Lessons from real-world experience. Australasian Psychiatry, 21(3), 258–261. https://doi.org/10.1177/1039856213475684
Myles, N., Myles, H., Xia, S., Large, M., Kisely, S., Galletly, C., Bird, R., & Siskind, D. (2018). Meta-analysis examining the epidemiology of clozapine-associated neutropenia. Acta Psychiatrica Scandinavica, 138(2), 101–109. https://doi.org/10.1111/acps.12898
Nordström, A. L., Farde, L., Nyberg, S., Karlsson, P., Halldin, C., & Sedvall, G. (1995). D1, D2, and 5-HT2 receptor occupancy in relation to clozapine serum concentration: a PET study of schizophrenic patients. The American journal of psychiatry, 152(10), 1444–1449. https://doi.org/10.1176/ajp.152.10.1444
Northwood, K., Pearson, E., Arnautovska, U., Kisely, S., Pawar, M., Sharma, M., Vitangcol, K., Wagner, E., Warren, N., & Siskind, D. (2023). Optimising plasma clozapine levels to improve treatment response: an individual patient data meta-analysis and receiver operating characteristic curve analysis. The British journal of psychiatry : the journal of mental science, 222(6), 241–245. https://doi.org/10.1192/bjp.2023.27
Pallares Vela, E., Dave, P., & Cancarevic, I. (2021). Clozapine-related thromboembolic events. Cureus, 13(8), e16883. https://doi.org/10.7759/cureus.16883
Patel, R. S., Veluri, N., Suchorab, A., Shah, K., & Verma, G. (2021). Clozapine-Induced Constipation: A Case Report and Review of Current Management Guidelines. Cureus, 13(5), e14846. https://doi.org/10.7759/cureus.14846
Puder, D. (Host). (2022, March 8). Psychopharmacology Mediators (No. 141) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/episode-141-psychopharmacology-mediators?rq=141
Puder, D. (Host). (2024a, May 29). Q&A with Dr. Cummings Part 2 (No. 214) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/episode-214-qanda-with-dr-cummings-part-2#:~:text=antagonist,treating%20me%20with%20something%20that
Puder, D. (Host). (2024,Sept. 27). Managing Weight Gain from Psychiatric Medications with Dr. Michael Cummings (No. 223) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/episode-223-glp1-agonists-for-psych-med-induced-weight-gain
Rogers, J. P., Oldham, M. A., Fricchione, G., Northoff, G., Ellen Wilson, J., Mann, S. C., Francis, A., Wieck, A., Elizabeth Wachtel, L., Lewis, G., Grover, S., Hirjak, D., Ahuja, N., Zandi, M. S., Young, A. H., Fone, K., Andrews, S., Kessler, D., Saifee, T., Gee, S., … David, A. S. (2023). Evidence-based consensus guidelines for the management of catatonia: Recommendations from the British Association for Psychopharmacology. Journal of psychopharmacology (Oxford, England), 37(4), 327–369. https://doi.org/10.1177/02698811231158232
Saini, A., Begum, N., Matti, J., Ghanem, D. A., Fripp, L., Pollak, T. A., Zandi, M. S., David, A., Lewis, G., & Rogers, J. (2024). Clozapine as a treatment for catatonia: A systematic review. Schizophrenia research, 263, 275–281. https://doi.org/10.1016/j.schres.2022.09.021
Segev, A., Iqbal, E., McDonagh, T. A., Casetta, C., Oloyede, E., Piper, S., Plymen, C. M., & MacCabe, J. H. (2021). Clozapine-induced myocarditis: electronic health register analysis of incidence, timing, clinical markers and diagnostic accuracy. The British journal of psychiatry : the journal of mental science, 219(6), 644–651. https://doi.org/10.1192/bjp.2021.58
Spivak, B., Mester, R., Abesgaus, J., Wittenberg, N., Adlersberg, S., Gonen, N., & Weizman, A. (1997). Clozapine treatment for neuroleptic-induced tardive dyskinesia, parkinsonism, and chronic akathisia in schizophrenic patients. The Journal of clinical psychiatry, 58(7), 318–322. https://doi.org/10.4088/jcp.v58n0706
Stanilla, J. K., de Leon, J., & Simpson, G. M. (1997). Clozapine withdrawal resulting in delirium with psychosis: A report of three cases. The Journal of Clinical Psychiatry, 58(6), 252–255. https://doi.org/10.4088/jcp.v58n0603
Taipale, H., Tanskanen, A., & Tiihonen, J. (2023). Safety of Antipsychotic Polypharmacy Versus Monotherapy in a Nationwide Cohort of 61,889 Patients With Schizophrenia. American Journal of Psychiatry, 180(5), 377–385. https://doi.org/10.1176/appi.ajp.20220446
Tanzer, T., Warren, N., McMahon, L., Barras, M., Kisely, S., Brooks, E., & Siskind, D. (2023). Treatment strategies for clozapine-induced nocturnal enuresis and urinary incontinence: A systematic review. CNS Spectrums, 28(2), 133–144. https://doi.org/10.1017/S1092852922000050
Taylor, C., Marsh-Davies, A., Skelly, R., Archibald, N., & Jackson, S. (2022). Setting up a clozapine service for Parkinson’s psychosis. BJPsych Advances, 28(2), 90–98. DOI: https://doi.org/10.1192/bja.2021.24
Tiihonen, J., Taipale, H., Mehtälä, J., Vattulainen, P., Correll, C. U., & Tanskanen, A. (2019). Association of Antipsychotic Polypharmacy vs Monotherapy With Psychiatric Rehospitalization Among Adults With Schizophrenia. JAMA psychiatry, 76(5), 499–507. https://doi.org/10.1001/jamapsychiatry.2018.4320
Varma, S., Bishara, D., Besag, F. M., & Taylor, D. (2011). Clozapine-related EEG changes and seizures: dose and plasma-level relationships. Therapeutic advances in psychopharmacology, 1(2), 47–66. https://doi.org/10.1177/2045125311405566
Wang, G., Zheng, W., Li, X.-B., Wang, S.-B., Cai, D.-B., Yang, X.-H., Ungvari, G. S., Xiang, Y.-T., & Correll, C. U. (2018). ECT augmentation of clozapine for clozapine-resistant schizophrenia: A meta-analysis of randomized controlled trials. Journal of Psychiatric Research, 105, 23–32. https://doi.org/10.1016/j.jpsychires.2018.08.002
Zhou, S. F., Wang, B., Yang, L. P., & Liu, J. P. (2009). Structure, function, regulation and polymorphism and the clinical significance of human cytochrome P450 1A2. Drug Metabolism Reviews, 42(2), 268–354. https://doi.org/10.3109/03602530903286476