
Episode 127: Using Antipsychotic Plasma Levels-Therapeutic Threshold
By listening to this episode, you can earn 1 Psychiatry CME Credits.
Other Places to listen: iTunes, Spotify
Article Authors: Joshua Salzman, Jonathan Meyer, MD, David Puder, MD
On this episode of the psychiatry and psychotherapy podcast, we are joined by psychiatrist, psychopharmacologist, and author, Dr. Jonathan Meyer, to talk about using antipsychotic plasma levels to assess treatment response, safety, and oral medication adherence. He is a clinical professor of psychiatry at the University of California, San Diego. He recently published a book with Dr. Stephen Stahl for clinicians to utilize called, The Clinical Use of Antipsychotic Plasma Levels: Stahl's Handbooks.
Dr. Meyer reports the following conflicts of interest:
Dr. Meyer reports having received advising fees in the prior 12 months from Acadia Pharmaceuticals, Alkermes, Intra-Cellular Therapies, Karuna, Neurocrine and Sunovion Pharmaceuticals.
Dr. Meyer reports having received speaking fees in the prior 12 months from Acadia Pharmaceuticals, Alkermes, Intra-Cellular Therapies, Neurocrine, Noven, Otsuka America, Inc., Sunovion Pharmaceuticals.
Based on our assessment, Dr. Meyer did not unduly mention or promote the associated medications in this episode. Dr. Puder and Joshua Salzman have no conflicts of interest to report.
Why Use Antipsychotic Plasma Levels?
When prescribing antipsychotics to people with schizophrenia, most clinicians use their past experience and training when approaching the ideal dose of an antipsychotic medication rather than drawing an antipsychotic level. Clinicians assess the need for dose adjustments clinically; they do this by observing a patient’s mental status, presence or absence of psychotic symptoms, and presence or absence of adverse effects from the chosen medication. Often this clinical approach to medication titration is not enough to achieve symptomatic response. One study of 99 people with schizophrenia who were thought to be treatment resistant and in need of clozapine showed that 35% had subtherapeutic plasma antipsychotic levels (McCutcheon, et. al, 2018).
This study illustrates how difficult it can be, in the absence of antipsychotic plasma levels, for clinicians to define treatment-resistant schizophrenia. Treatment-resistant individuals are patients who have failed multiple trials of different antipsychotic medication. There are several reasons that are often overlooked by clinicians that patients “fail” a trial of a medication. Patients could be nonadherent, underdosed, or rapidly metabolize the antipsychotic due to genetic reasons or the presence of enzyme inducers (McCutcheon et.al, 2015).
Antipsychotic nonadherence is common in patients with schizophrenia and, unfortunately, clinicians are poor estimators of nonadherence (Dufort and Zipursky, 2019, Brian et. al, 2014) Byerly et. al, 2007, Lopez et.al, 2017). How does one mitigate the issues of nonadherence, underdosing, and genetic variations in drug metabolism? One strategy is to utilize plasma antipsychotic levels and therapeutic thresholds.
What is a therapeutic threshold?
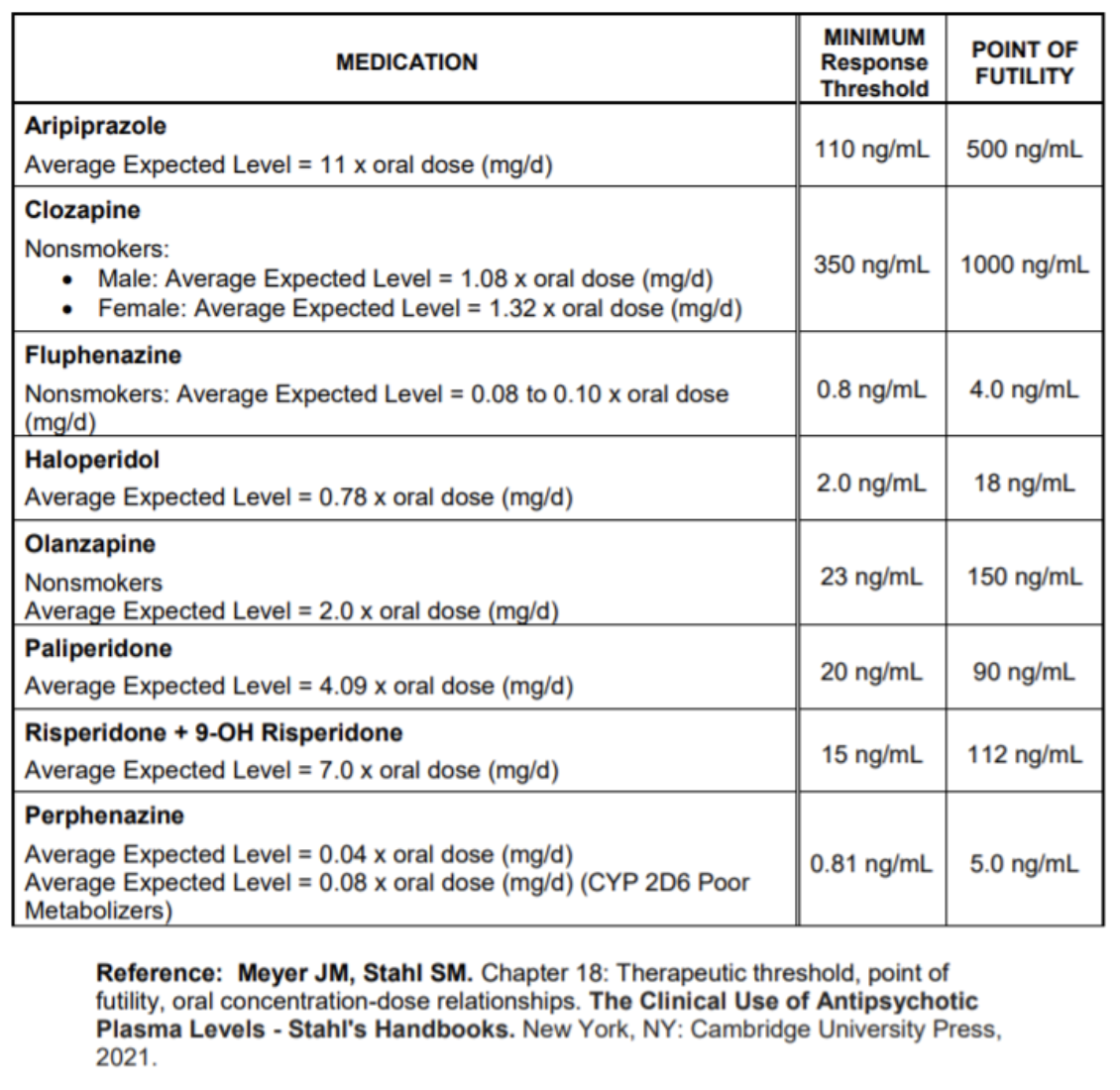
The therapeutic threshold for antipsychotics is “a plasma level of the medication that best differentiates true responders from non-responders” (Meyer and Stahl, 2021).
What are responders and nonresponders?
Per the recent literature for acute psychosis trials, a response is defined as 50% symptom reduction (Samara et al., 2015).
Some patients may respond significantly below the response threshold. For mental health providers, the therapeutic threshold represents an initial target plasma level for patients who are “inadequate responders who do not experience dose-limiting adverse effects” (Meyer, 2021).
How Reliable are Genetic Tests in Measuring who are Responders vs. Nonresponders?
Providers may ask: “Why not just check a patient’s CYP450 genetic metabolic profile?”
When genetic panels were released, they were thought to give hope for many patients to better understand their individualized response to medication. To date, the panels continue to utilize polymorphisms that were identified over a decade ago (Meyer, 2021). Since the discovery and commercial utilization of these polymorphisms, several new alleles have been discovered. Unfortunately the genetic panel companies have not been able to update their panels with these newly identified alleles. Therefore, when a patient receives a genetic panel and their report says “extensive metabolizer at CYP2D6”, misleading information may be provided to the clinician and patient. People also are not “single gene” metabolizers and have multiple polymorphisms that contribute to their metabolism of certain medications (Ruan and de Leon, 2020). Furthermore, the genetic panels do not consider the external factors that influence a patient’s response to medication such as: medicines that act as metabolic inhibitors or inducers, variable absorption of medication, how our renal system processes medications, medication adherence, or overdosing on medication. Plasma levels provide the clinician with the specific information (i.e., the drug level) which accurately reflects the sum total of all these interacting factors (Ruan and de Leon, 2020).
D2 Occupancy and PET Scans:
The literature has shown a correlation between the percentage of D2 receptor occupancy for typical antipsychotics and treatment efficacy. For antipsychotics whose presumed mechanism is D2 antagonism, PET scans obtained at steady state show a range of occupancy thresholds for an adequate antipsychotic response from 50% to 65%. The lower values come from studies of first-episode schizophrenia patients, but 60%-65% are the most commonly cited values for chronic schizophrenia (Uchida et al. ,2011, Arkawa et al.,2020, de Haan et al. 2003). After surpassing the threshold of 80% D2 occupancy, the risks of adverse neurological effects (e.g., parkinsonism, akathisia, dystonia) increase. The “sweet spot” for D2 occupancy is between 65%-80% (Meyer, 2021).
Issues with partial agonists: Aripiprazole, brexpiprazole & cariprazine have varying levels of intrinsic dopamine activity and operate at 80%-100% D2 occupancy (Meyer, 2021).
Issues with other antipsychotics: clozapine and lumateperone work with extremely low levels of D2 occupancy, so the correlation between response and occupancy does not hold (Meyer, 2021).
How Can Mental Health Providers Use Therapeutic Thresholds Clinically?
They can use them to assess if the patient is receiving minimally effective antipsychotic exposure when there appears to be a lack of response.
They can use them to assess if a patient has a high level when they are experiencing adverse effects, or to decide when further dose and plasma levels increase are unlikely to benefit the patient, and will push the level beyond the point of futility where the chances of response are < 5%.
They can use them to assess an accidental or intentional overdose.
They can use them to address medication nonadherence (Meyer, 2021).
We must clarify several questions when discussing a patient’s plasma level, accidental overdose, and medication nonadherence:
Is the patient taking multiple doses?
In order to improve adherence, providers should aim to utilize once daily dosing and minimize changes to the patient’s regimen (Pfeiffer, Ganoczy, and Valenstein, 2008).
What does the objective data tell the provider?
The current evidence-based strategies show that inquiring about prescription refills, receiving 3rd party information, scheduling home visits with unannounced pill counts, and ordering plasma antipsychotic levels are effective strategies to gather objective data (Velligan et al., 2007).
It is important to not assume or infer any level of adherence based on the provider’s perceived patient stability or what the patient self-reports (Meyer, 2021).
How do we remind the patient to take their medication?
Providers may utilize every tool available to them “(e.g., reminders via text, phone or email; timed pill boxes with alerts) despite literature suggesting modest benefits” (Nieuwlaat et al., 2014, Beebe, Smith, Phillips, 2017, Xu et al., 2019, Uslu and Buldukoglu, 2020).
How can providers communicate effectively?
It is important to normalize nonadherence to uncover the entirety of the patient’s struggle with compliance (McCabe et al., 2013).
Framing nonadherence in a nonjudgmental way has shown to be an effective way of inquiry such as: “Most people who take medicines every day miss some doses. How many do you think you missed in the past 4 weeks?” rather than offering a question such as “Did you take your pills?” to which the answer will uniformly be “Yes” (Meyer, 2021).
It is important to gauge the patient’s attitudes toward their treatment. Providers should openly and nonjudgmentally solicit explanations and concerns that relate to the patient’s noncompliance. Providers should aim to “utilize shared decision-making principles as much as possible” (McCabe et al., 2013, Gaebel et al., 2010, Quirk et al., 2010).
Is nonadherence common?
50% of patients with any chronic conditions, whether psychiatric in nature or not, struggle with oral medication adherence (Lam and Fresco, 2015, Abegaz et. al, 2017 ).
Providers should be aware that medication nonadherence is a “common, persistent and pervasive issue” (Meyer, 2021).
It is important to “not become complacent, regardless of your level of expertise” (Kurokawa et al., 2019).
Providers should aim to understand that “medication adherence is dynamic and changes over time” (MacEwan et al., 2016).
My patient has an antipsychotic level above the therapeutic threshold...now what?
Having a plasma level above the therapeutic threshold is no guarantee of response. Assuming tolerability, the plasma level should be titrated in nonresponders until one of 3 endpoints are reached (Meyer and Stahl, 2021):
The patient has improved significantly and is a responder.
The patient experiences dose limiting adverse effects.
The “point of futility” is reached.
What is the “point of futility” (Meyer, 2021)?
The point of futility is a term devised to provide clinicians a single upper limit value, and to educate clinicians about two important concepts (Meyer, 2014):
1) Often, when a patient can no longer tolerate an antipsychotic’s adverse effects, this is a sign to end an antipsychotic trial. A small number of patients may never experience dose-limiting adverse effects and others will tolerate further antipsychotic titration to higher doses, even with high potency first generation antipsychotics ( Simpson and Kunz-Bartholini, 1968).
2) Although a patient may be able to tolerate higher doses of a drug trial, titrating beyond a certain plasma level (the point of futility) is futile, “as less than 5% of patients will respond to these higher plasma levels” (Meyer, 2014, Midha et al., 1994).
Do different labs report varying plasma level ranges?
Unfortunately, clinicians and their patients may see inconsistent ranges of antipsychotic levels reported from different lab drawing services. This is a problem that appears unique to antipsychotics; such wide variations are not seen for mood stabilizers such as lithium and valproate. These discrepancies in lab reporting of antipsychotic therapeutic ranges can cause concern and confusion for the treating clinician; at times, this may result in an inappropriate reaction to an elevated or lowered antipsychotic level (Meyer and Stahl, 2021).
For example as of July, 2020:
Quest Labs reports a therapeutic range for Haloperidol: 5-15ng/mL, while LabCorp reports a therapeutic range for Haloperidol: 1-10 ng/mL.
ARUP reports that the toxic haloperidol level is > 42.0 mg/mL, while LabCorp reports a potentially toxic haloperidol level is > 50.0 mg/ml.
How do we respond to high antipsychotic levels?
When we see elevated antipsychotic levels, our primary concern is to evaluate the patient's safety. We assess a patient’s safety through clinical evaluation. Many clinicians become alarmed when high levels are reported; as a reaction to this, providers may reduce doses without first determining whether the elevated level is congruent with the clinical picture. Most patients with high plasma levels typically show adverse effects consistent with the level. Furthermore, as noted above, there is wide variation in what laboratories refer to as a high antipsychotic level (Meyer, 2021, Meyer 2019).
Before any action to lower a dose or discontinue a patient’s medication, a few steps need to be performed:
Steps to Evaluate A Patient’s Elevated Antipsychotic Level (Meyer, 2021):
When approaching an elevated antipsychotic level, it is best to explore this finding with the patient themself. Ideally, they should be seen in the clinic, in person. If the patient cannot attend the clinic, then they may be contacted by phone or telemedicine. The goal of this encounter is to assess the patient’s changes in their response to their medication. The clinician should explore if the patient is experiencing new adverse effects or changes in severity of preexisting adverse effects.
If a patient is receiving divided daily oral doses, explore with the patient if the morning dose was accidentally given prior to the patient’s blood draw.
If a patient is taking an oral antipsychotic, determine if the level was drawn at a “12hr ± 2hr trough” (Meyer, 2021). If the patient is on a LAI, explore “whether the level was obtained at peak concentrations based on the specific kinetics of that preparation, or if it was drawn at trough levels 1 hr-72hr prior to the next scheduled dose” (Meyer, 2021).
It is imperative to assess whether the intended oral dose was in fact ingested, or whether there was an accidental or intentional overdose. Clinicians must lean on their therapeutic alliance with their patients to investigate an accidental or intentional overdose of their medication. If the patient is prescribed an LAI, assess whether the intended doses were administered and then explore the recent schedule of injections.
Review all of the patient’s active psychiatric and nonpsychiatric medications to determine whether a metabolic inhibitor, like a CYP450 inhibitor, was recently added, or whether a metabolic inducer was recently discontinued.
In Conclusion, Utilizing Plasma Levels Helps Providers and Patients.
Plasma levels offer providers an objective marker to assess a patient’s response to an antipsychotic medication. They help inform mental health providers if the patient is adherent to their regimen and conclude how the patient is breaking down the medication. A plasma level also offers the provider information if the patient is receiving an adequate dose, or receiving too high a dose. Providers routinely draw Lithium or Valproic Acid levels to assess a patient’s therapeutic response and safety profile- why not draw antipsychotic levels? The provider may use the patient’s plasma level to adjust the current dose and understand a patient’s reasons for possible medication nonadherence. Providers should lean on their therapeutic alliance with their patient and align their goals. If this is achieved, antipsychotic adverse effects can be minimized and the patient’s treatment response can be optimized.
For those of you interested, you can find Dr. Meyer’s book here.
References:
Arakawa, R., Takano, A., & Halldin, C. (2020). PET technology for drug development in psychiatry. Neuropsychopharmacology Reports, 40(2), 114-121.
https://onlinelibrary.wiley.com/doi/full/10.1002/npr2.12084
Beebe, L. H., Smith, K., & Phillips, C. (2017). Effect of a telephone intervention on measures of psychiatric and nonpsychiatric medication adherence in outpatients with schizophrenia spectrum disorders. Journal of psychosocial nursing and mental health services, 55(1), 29-36.
Brain, C., Sameby, B., Allerby, K., Lindström, E., Eberhard, J., Burns, T., & Waern, M. (2014). Twelve months of electronic monitoring (MEMS®) in the Swedish COAST-study: a comparison of methods for the measurement of adherence in schizophrenia. European Neuropsychopharmacology, 24(2), 215-222.
Byerly, M. J., Thompson, A., Carmody, T., Bugno, R., Erwin, T., Kashner, M., & Rush, A. J. (2007). Validity of electronically monitored medication adherence and conventional adherence measures in schizophrenia. Psychiatric Services, 58(6), 844-847.
https://ps.psychiatryonline.org/doi/full/10.1176/ps.2007.58.6.844
de Haan, L., van Bruggen, M., Lavalaye, J., Booij, J., Dingemans, P. M., & Linszen, D. (2003). Subjective experience and D2 receptor occupancy in patients with recent-onset schizophrenia treated with low-dose olanzapine or haloperidol: a randomized, double-blind study. American Journal of Psychiatry, 160(2), 303-309.
Dufort, A., & Zipursky, R. B. (2019). Understanding and Managing Treatment Adherence in Schizophrenia. Clinical schizophrenia & related psychoses.
Gaebel, W., Riesbeck, M., von Wilmsdorff, M., Burns, T., Derks, E. M., Kahn, R. S., ... & EUFEST Study Group. (2010). Drug attitude as predictor for effectiveness in first-episode schizophrenia: results of an open randomized trial (EUFEST). European Neuropsychopharmacology, 20(5), 310-316.
Iyo, M., Tadokoro, S., Kanahara, N., Hashimoto, T., Niitsu, T., Watanabe, H., & Hashimoto, K. (2013). Optimal extent of dopamine D2 receptor occupancy by antipsychotics for treatment of dopamine supersensitivity psychosis and late-onset psychosis. Journal of clinical psychopharmacology, 33(3), 398-404.
Kurokawa, S., Kishimoto, T., Su, K. P., Chang, J. P. C., Chang, H. C., Yu, X., ... & Kane, J. M. (2019). Psychiatrists' perceptions of medication adherence among patients with schizophrenia: An international survey. Schizophrenia research, 211, 105-107.
Lopez, L. V., Shaikh, A., Merson, J., Greenberg, J., Suckow, R. F., & Kane, J. M. (2017). Accuracy of clinician assessments of medication status in the emergency setting: a comparison of clinician assessment of antipsychotic usage and plasma level determination. Journal of clinical psychopharmacology, 37(3), 310-314.
MacEwan, J. P., Forma, F. M., Shafrin, J., Hatch, A., Lakdawalla, D. N., & Lindenmayer, J. P. (2016). Patterns of adherence to oral atypical antipsychotics among patients diagnosed with schizophrenia. Journal of managed care & specialty pharmacy, 22(11), 1349-1361.
McCutcheon, R., Beck, K., Bloomfield, M. A., Marques, T. R., Rogdaki, M., & Howes, O. D. (2015). Treatment resistant or resistant to treatment? Antipsychotic plasma levels in patients with poorly controlled psychotic symptoms. Journal of Psychopharmacology, 29(8), 892-897.
https://journals.sagepub.com/doi/abs/10.1177/0269881115576688
McCutcheon, R., Beck, K., D'Ambrosio, E., Donocik, J., Gobjila, C., Jauhar, S., ... & Howes, O. D. (2018). Antipsychotic plasma levels in the assessment of poor treatment response in schizophrenia. Acta Psychiatrica Scandinavica, 137(1), 39-46.
https://onlinelibrary.wiley.com/doi/full/10.1111/acps.12825
Meyer, J. M. (2014). A rational approach to employing high plasma levels of antipsychotics for violence associated with schizophrenia: case vignettes. CNS spectrums, 19(5), 432-438.
https://www.cambridge.org/core/journals/cns-spectrums/article/abs/rational-approach-to-employing-high-plasma-levels-of-antipsychotics-for-violence-associated-with-schizophrenia-case-vignettes/E83BC92675B01F183A86BFBA4523BD5C
Meyer, J. M., & Stahl, S. M. (2019). The Clozapine Handbook: Stahl's Handbooks. Cambridge University Press.
https://books.google.com/books?hl=en&lr=&id=8LOQDwAAQBAJ&oi=fnd&pg=PR9&dq=.+Meyer+JM,+Stahl+SM.+The+Clozapine+Handbook.+Cambridge,+UK:+Cambridge+University+Press%3B+2019.&ots=SVWzoC-1mB&sig=ZtVeXqFiPNoKRflek6kVzXZOEtw#v=onepage&q&f=false
Meyer, J. M. (2020). Monitoring and improving antipsychotic adherence in outpatient forensic diversion programs. CNS spectrums, 25(2), 136-144.
Meyer, J. M., & Stahl, S. M. (2021). The Clinical Use of Antipsychotic Plasma Levels: Stahl's Handbooks. Cambridge University Press.
https://books.google.com/books?hl=en&lr=&id=-pNBEAAAQBAJ&oi=fnd&pg=PT9&dq=Meyer+JM,+Stahl+SM.+The+Clinical+Use+of+Antipsychotic+Plasma+Levels+-+Stahl%E2%80%99s+Handbooks.+New+York:+Cambridge+University+Press%3B+2021.&ots=Q0dUg1xGap&sig=H6fW45D7mjNeTuG8LZmiep-x80Y#v=onepage&q&f=false
Midha, K. K., Hubbard, J. W., Marder, S. R., Marshall, B. D., & Van Putten, T. (1994). Impact of clinical pharmacokinetics on neuroleptic therapy in patients with schizophrenia. Journal of Psychiatry and Neuroscience, 19(4), 254.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1188605/
Nieuwlaat, R., Wilczynski, N., Navarro, T., Hobson, N., Jeffery, R., Keepanasseril, A., ... & Haynes, R. B. (2014). Interventions for enhancing medication adherence. Cochrane database of systematic reviews, (11).
Pfeiffer, P. N., Ganoczy, D., & Valenstein, M. (2008). Dosing frequency and adherence to antipsychotic medications. Psychiatric Services, 59(10), 1207-1210.
https://www.jmcp.org/doi/full/10.18553/jmcp.2016.22.11.1349
Quirk, A., Chaplin, R., Hamilton, S., Lelliott, P., & Seale, C. (2013). Communication about adherence to long-term antipsychotic prescribing: an observational study of psychiatric practice. Social psychiatry and psychiatric epidemiology, 48(4), 639-647.
Ruan, C. J., & de Leon, J. (2020). Is there a future for CYP1A2 pharmacogenetics in the optimal dosing of clozapine?.
Samara, M. T., Leucht, C., Leeflang, M. M., Anghelescu, I. G., Chung, Y. C., Crespo-Facorro, B., ... & Leucht, S. (2015). Early improvement as a predictor of later response to antipsychotics in schizophrenia: a diagnostic test review. American journal of psychiatry, 172(7), 617-629.
https://ajp.psychiatryonline.org/doi/full/10.1176/appi.ajp.2015.14101329
Simpson, G. M., & Kunz-Bartholini, E. (1968). Relationship of individual tolerance, behavior and phenothiazine produced extrapyramidal system disturbance. Diseases of the nervous system, 29(4), 269-274.
https://pubmed.ncbi.nlm.nih.gov/5652493/
Servonnet, A., & Samaha, A. N. (2020). Antipsychotic-evoked dopamine supersensitivity. Neuropharmacology, 163, 107630.
Uchida, H., Takeuchi, H., Graff-Guerrero, A., Suzuki, T., Watanabe, K., & Mamo, D. C. (2011). Predicting dopamine D2 receptor occupancy from plasma levels of antipsychotic drugs: a systematic review and pooled analysis. Journal of clinical psychopharmacology, 31(3), 318-325.
https://journals.lww.com/psychopharmacology/Abstract/2011/06000/Predicting_Dopamine_D2_Receptor_Occupancy_From.9.aspx
UsluUslu, E., & Buldukoglu, K. (2019). Randomized controlled trial of the effects of nursing care based on a telephone intervention for medication adherence in schizophrenia. Perspectives in psychiatric care, 56(1), 63-71.
Velligan, D. I., Wang, M., Diamond, P., Glahn, D. C., Castillo, D., Bendle, S., ... & Miller, A. L. (2007). Relationships among subjective and objective measures of adherence to oral antipsychotic medications. Psychiatric Services, 58(9), 1187-1192.
Xu, D., Xiao, S., He, H., Caine, E. D., Gloyd, S., Simoni, J., ... & Gong, W. (2019). Lay health supporters aided by mobile text messaging to improve adherence, symptoms, and functioning among people with schizophrenia in a resource-poor community in rural China (LEAN): A randomized controlled trial. PLoS medicine, 16(4), e1002785
Yada, Y., Kitagawa, K., Sakamoto, S., Ozawa, A., Nakada, A., Kashiwagi, H., ... & Yamada, N. (2021). The relationship between plasma clozapine concentration and clinical outcome: a cross‐sectional study. Acta Psychiatrica Scandinavica, 143(3), 227-237.
Acknowledgements:
This article was supported by “Mental Health Education & Research”.