
Episode 125: Treating the VIP: Physicians and the Famous or Wealthy
By listening to this episode, you can earn 1 Psychiatry CME Credits.
Other Places to listen: iTunes, Spotify
Article Authors: David Puder, MD
In this episode, Dr. Puder and Dr. Heacock discuss the complicating factors of treating physicians, the famous, and the wealthy.
David Puder M.D. and Craig Heacock, M.D have no conflicts of interest to report. Dr. Heacock is the host of a podcast called: “Back from the Abyss”
What is a VIP?
Very Important Patients are individuals who may be likely to receive special treatment from medical facilities or staff due to their influence or high societal standings. They could be colleagues who also practice medicine, or people that we have looked up to and admired. There is a real danger of medical professionals treating or behaving differently with someone they perceive to be a VIP, which leads to inferior treatment. For example, if a provider refuses to ask a VIP necessary questions because they could make the VIP feel uncomfortable or embarrassed, they may miss key information. Ultimately, it can be hard to empathize with a VIP because we may be too in our own experience of fears or internal dialogue, taking us away from offering the normal high level of care we give.
It is common to desire to give different care to people we see as having high influence, wealth, or that may be very similar to us in some way. A survey was conducted in Connecticut where 97% of medical directors approved of VIP treatment under the belief that it was “expediting care, not providing different care…” (Smalley et al 2011). At times, there are perceived secondary gains from treating these people as special, such as:
“I ask those who oppose the practice if they have an objection to expediting care for their family or staff's family or friends. We do that all the time without a big moral discussion. This is about control, not a concern for other patients. These folks are part of the larger hospital family” (Smalley et al 2011).
“I'd rather have these heavyweights complementing rather than complaining about my department to the CEO. Plus they can be very influential in terms of projects, improvements, and the flow of capital dollars towards areas they appreciate” (Smalley et al 2011).
What is Best for the VIP?
Often, VIPs reach out with special requests. They ask that rules be bent or broken for them and can have expectations of exceptional treatment. Remaining objective by focusing on what is best for the patient, and not on simply pleasing the patient by agreeing to these requests, ensures that they have the best chance of receiving the appropriate and necessary care.
A point worth noting is that VIPs often ask to be seen immediately. This may look like asking for an appointment after hours or specifically requesting a Zoom session because it is more convenient for them than being seen in person. These may seem like inconsequential favors to accommodate, but we must ask ourselves if this would mean they would receive subpar care. Seeing patients late in the day means we are tired and may have trouble being fully present. If we know a patient would benefit from an in-person session, agreeing to an online session could prevent them from having the most impactful session possible.
As psychiatrists, we can ask ourselves some questions in these scenarios to assess our objectivity:
What is best for the patient in this scenario?
Why am I saying yes or no?
What are my motives?
Am I keeping the treatment parameters the same as with my other patients?
Triggering Narratives Behind Treating VIPs
It is possible to walk into the treatment of a VIP with a past narrative that we subconsciously apply to the situation. We may pick up on a profound insecurity within the VIP and it can lead us to apply our own insecurities, such as our ability to provide them with sound treatment or if they respect our field of medicine, to our interpretation of the exchange. This is usually triggered by the more difficult VIP patients, often physicians, and makes it difficult to give them optimal treatment because instead of seeing the situation objectively, we are playing out our own scenarios.
Identifying these narratives and self-criticisms is crucial to providing the VIP with the best care. One way we can determine the clarity of our thoughts is imagining the scenario without these conscious thoughts. If the thoughts were not constantly registering in our consciousness, how could we reinterpret what was happening? Where we may first have interpreted that the patient does not respect us, we may, instead, reinterpret that the patient is very uncomfortable with seeing a psychiatrist for the first time and has some resistance to treatment.
Physician on Physician Care
There is an irony about physician on physician care. On one hand, physicians, as well as ourselves, can often desire to be seen as special and treated according to our professional status. Stemming all the way from childhood, a desire to feel noticed for what we do can follow us into adulthood. When we do not receive this treatment, such as receiving a very routine exam that doesn’t take into account our medical knowledge or experience, we can become agitated and frustrated. Being able to provide unbiased care, however, is a mark of maturity in the medical provider.
On the other hand, it may be generally assumed that a physician seeking treatment automatically receives this superior, expedited care, but many times the exact opposite occurs. Medical providers, especially the younger, greener providers, can easily become intimidated by the status of the physician and shy from giving them the care they truly need out of fear or embarrassment. Perhaps they assume, because of the physician’s medical knowledge, they don’t necessarily need the depth of care they are requesting.
We can ultimately all relate to the desire to be treated with the same level of care as any other person, and that should be something we strive for in our own practices.
The Categories of VIPs and How They Can Uniquely Influence Providers
Physicians
Doctors are often the hardest VIPs to treat because, as medical professionals ourselves, we identify with them. Physicians may know just enough psychiatry to believe they understand what treatment is warranted, which can blur the lines of therapeutic alliance, affect our ability to remain objective in our diagnosis, and potentially lead to the patient’s opinion of their treatment overriding our medical expertise (Alfandre et al 2016). We often have a high respect for these professionals and it can be difficult to overcome the notion of feeling inferior to their realm of specialities. It is imperative to remember that while they are well trained in their specialty, they do not have competency in psychiatry; that is why they come to us.
Another challenge with treating physicians is that, by and large, they are very hesitant to seek treatment for mental health issues, often not showing up at our offices until their health has declined into something serious, such as suicidal thoughts.
Barriers for physicians to seek treatment:
Board Requirements
Knowing that medical licensing board requirements ask questions about their mental health and whether they have ever sought treatment in the past or taken medications for mental health issues.
One survey showed that 75% of physicians cited that medical licensing board questions prevented them from seeking treatment.
Shame
Often these high-achieving VIPs are operating from a place of shame, potentially compensating for the feeling that they did not live up to certain expectations as a child.
This same shame can influence their ability to admit they need help with their mental health.
The fear of not being able to work
This is very prevalent among physicians and they often only seek help once their situation is quite dire.
How we can encourage VIP physicians to seek treatment:
Discuss note taking.
Let them know that there are times you don't have to include certain things in your notes.
However, the other side of that coin is we cannot avoid asking the hard or embarrassing questions that may have to be reported to medical boards or may promote our own transference if the VIP is in our same field.
Consider the risk of keeping their records in a cloud.
Knowing that there is not a trail of their medical records that other offices can access can offer comfort.
Promote the benefits of seeking care early.
Celebrities
Celebrities are most likely the easiest VIPs to recognize. Their lives are constantly in public view which makes them susceptible to VIP syndrome. The VIP status can be given to negative celebrities as well; this would include individuals who are well known due to their criminal activity.
Celebrity VIPs can be difficult to navigate for several reasons:
Celebrities may assume they will receive special treatment in a similar fashion to how others treat them outside of the medical community.
VIPs may assume the doctor already knows why they’re looking for a medical professional due to the innate publicity of their lives. As such, they may not divulge crucial information, assuming it is already known (Gainer and Cowan 2019).
Physicians may have trouble keeping objectivity in care by trying to impress the celebrity, or they might avoid asking important questions to avoid embarrassing the patient.
Ensuring privacy is maintained can be a major hurdle, including setting boundaries with the VIP’s entourage, who are used to completing paperwork or making appointments for the celebrity.
The Wealthy or Influential
Special status can be given to any wealthy or influential person even if they are not known to the public at large. For example, a physician or board member who is well known and greatly admired in a medical facility could easily fall into the VIP category. Known donors could also be a potential cause for VIP syndrome if the staff fear they might lose financial support if they don’t go above and beyond the standard care.
Chairperson Syndrome
“Chairperson Syndrome” is also a possible issue within influential VIPs. This occurs when a department chair or an individual who ranks highly in the medical facility is chosen to be the primary physician due to their status. Instead, physicians should always be chosen based on their qualifications to handle the ailments affecting the patient regardless of their social status. The department chair should only be the VIP’s primary physician if they are the best suited for the patient’s needs (Guzman et al 2011).
Potentates
Potentates are slightly different from the previous categories because the VIP status is viewed from the patient’s perspective rather than the physician’s. Potentates often exhibit narcissistic traits, which reveal themselves in an attitude of supreme importance and expectation that others should give them special treatment (Groves et al 2002). They might have a much higher self-projected image of themselves than any competence or history would validate. Even though this is often a one-sided view, potentates will treat medical staff members as inferior through the display of contemptuous ingratitude.
“Potentates are individuals whose grandiosity and contempt for others are buttressed by actual power in the world. Sometimes this power derives from talent or industry; sometimes, just luck. Despite whatever appears on the surface though, at the deepest level, such individuals are full of shame. They are terrified of being found out and exposed as impostors. Their effort to promote a grandiose image is typically to reassure themselves or to provide a distraction from intense anxiety. Because of their stunted or absent empathy, they make bad spouses, bad friends, bad parents, and bad patients” (Groves et al 2002).
Common Pitfalls of Treating a VIP
Transference
VIPs may desire or expect VIP treatment (off-hour appointments, very quick emergency appointments, visits to their home).
VIPs may treat psychiatrist as a friend/peer rather than a medical professional (Gainer and Cowan 2019).
VIPs may desire a quick solution and see you as a God-like figure who will make it happen.
VIPs may question your competence and inability to cure them quickly.
Countertransference
When handling VIPs, it is possible to give into often false narratives (based on fears of inadequacy or being an imposter) that the patient won’t take the physician seriously or that the patient thinks of themselves more highly than the physician. Insecurities or past experiences can come to mind when dealing with VIPs, which could cloud one’s judgement or the experience with the patient. It’s important to recognize these narratives and then determine if it is something that the patient is actually conveying or if countertransference is taking place within the interaction.
Three possible countertransference with VIP patients
Mirroring countertransference (desire to be liked and wanting to please the patient)
Loss of objectivity
Fear of rejection/retribution
Fear of inadequacy
Idealizing countertransference (looking up to or idealizing the patient)
Avoiding difficult aspects of the VIP’s history
Not ask about drug or alcohol use or sexual dysfunction
Misinterpreting therapeutic dialogue to maintain the idealization (Gainer and Cowan 2019)
Dichotomous thinking
Striving for unachievable outcomes in order to rescue the VIP while also dreading failing the VIP (Gainer and Cowan 2019)
The Effects on Nurses
When it comes to VIP Syndrome, most of the concern surrounds the relationship between the patient and the physician. However, nurses are just as likely to feel pressured into giving special treatment to VIPs. In one study, it was reported that “...one-third of the 160 hospitalists surveyed reported feeling pressure from the hospital staff to provide special treatment to VIP patients” (Perrone 2020). The urge to give special treatment to those individuals with high social status is most likely due to the benefits hospitals receive when a VIP has a positive experience at their location. The notoriety given to the medical staff for taking care of a VIP is essentially the same as getting a celebrity endorsement. On other hand, if a VIP has a terrible experience, the reputation of the staff and facilities could be under severe scrutiny, which only adds to the temptation to give VIPs special treatment.

Gifts
Gifts can be difficult to navigate, especially if VIPs are disconnected from the value of the gifts given. For them, the gift may seem like a small gesture, but for those who don’t have nearly the same amount of wealth, the gift is profound (Gainer and Cowan 2019). An obvious concern in gift giving is the possible ulterior motive affiliated with it. Physicians may be putting themselves in a vulnerable position if the accepting of gifts comes with the expectation that the VIP’s opinions/desires will be taken into account over more objective treatment.
Gifts could also come with an underlying expectation of receiving special treatment. Of course, gifts could be given out of the generosity of the VIP, but it’s still risky to take such gifts, especially with high profile clients. Gifts affect more than just the physician; gifts given to staff could certainly alter the treatment given to VIPs. Overall, it is better to kindly reject any gifts offered in order to ensure the medical staff remains objective in their treatment of VIPs, as well as making sure there aren’t any misunderstandings within the doctor/patient relationship.
Charisma and Confidence
There are individuals who have such a natural charisma and warmth that it creates an immediate kinship that could block the objectivity necessary to give proper treatment. It could lead a physician to accept requests by the patient, such as medications asks, that they wouldn’t ordinarily prescribe, especially when a patient is confident and charismatic. This is not to say a VIP in this category is using manipulative tactics to get what they want, but it’s possible that a patient may be so warm and charismatic that a medical professional, consciously or unconsciously, gives in to their demands because of their innate ability to connect with people quickly, including their doctors.
Points of VIP Resistance
In-person treatment
VIPs often lead busy lives that compound on a culture of quick fixes, which may lead to requests of being treated over a quick phone call or text message. Medical professionals also have full schedules, which might make it tempting to cut corners by giving quick or convenient care to these VIPs. However, medical professionals must give the best care possible, not necessarily the easiest or most convenient care. A good rule of thumb is that if you wouldn’t treat a regular patient in the way a VIP is asking you to treat them, you should not do it.
Commitment to the weekly work of therapy
This often comes down to the management of shame. Shame is a powerful hurdle when it comes to getting the necessary help that someone needs. It can be easy for outsiders to assume a VIP doesn’t experience shame. It is crucial to understand that success in one’s life does not mean the absence of shame. Some of the hardest- working people are hard working because of the amount of shame they experienced (or don’t want to experience). Creating an environment where a patient can talk about the shame they feel can be a major stepping stone to increasing their commitment to therapy.
Lack of understanding the value of therapy
The journey to mental stability is far more often a marathon rather than a sprint. The benefits of therapy are not always immediately noticeable and this can lead to two notable problems. First, the patient might become impatient due to their expectation of a quick fix and desire to move on with their lives. This is possibly the reason a study found that physician autopsies revealed a rate of benzodiazepines at an odds ratio of 21 compared to the general population (Gold 2013).
The second issue is a patient might mistakenly attribute the benefits resulting from therapy to something else. Perhaps they believe the newfound stability in their lives is due to their diet or medications they have received rather than the time spent in therapy. If the patient can’t see the long term benefits of therapy or see it as the source of their mental stability, they may find it difficult to continue the important work of therapy on a weekly basis.
Getting Resistant Patients to Therapy
Spousal involvement
If the patient is married, it can be helpful to get their spouse involved to encourage therapy compliance. The patient may not be able to see how unhealthy they have become or might downplay their problems. Bringing in a spouse can help the patient see how their behavior is affecting their daily lives, as well as the lives of those who depend on them. It’s also helpful to have spousal involvement so the patient has someone else encouraging them to get the help that they need.
Being up front about the possible pitfalls and difficulties
When dealing with a VIP, especially another medical professional, it is crucial to be open about the possibility of special treatment being given or a lack of objectivity. Openly communicating about such pitfalls can create rapport between the patient and therapist as well as create a mutual accountability that will keep both parties on the lookout for pitfalls.
Willingness to be appropriately vulnerable
Medical professionals should always have boundaries with their patients. It’s important for professionals to be wary of taking away from therapy time by disclosing too much about their own problems. However, there might be moments where it is appropriate to share a little bit in order to build trust with patients, as well as to let them see that medical professionals are not immune to the ills of the world.
An example of this would be a therapist who finds themselves yawning frequently throughout a session. A vulnerable patient might believe that the yawns are due to boredom, in which case it might be beneficial for the therapist to mention that they have been experiencing extra burdens in their life, which has kept them from getting the amount of sleep they would like. This both informs the patient that the yawning has nothing to do with them while simultaneously showing vulnerability.
Real Life Examples of VIP Syndrome Gone Awry
One major difficulty in treating VIP patients is that they are not accustomed to being in a position where they are not in control, which can make it difficult for them to take medical advice they do not want.
When medical systems that are in place for the protection of the patient are bypassed, it increases the chance of harming the patient and a potential subsequent malpractice suit.
Joan Rivers’ clinic/doctors took responsibility in a malpractice lawsuit after the comedian died in a routine procedure due to the doctors being overwhelmed by the star's presence. In 2014, one doctor took a photo of Rivers while she was on the operating table, which is a major violation of protocols (Carroll 2016).
Michael Jackson’s doctor was convicted of involuntary manslaughter for prescribing propofol at the request of the patient to help him sleep in 2009 (Carroll 2016).
Steve Jobs refused to let doctors remove a pancreatic tumor hoping to find alternative medicinal remedies. By the time he finally gave in to the physician's request, the tumor had spread out of control (Carroll 2016).
Six employees were fired for illegally accessing the medical records of Kim Kardashian while she was in the hospital on June 15, 2013 (McCann 2013).
Mickey Mantle, a famous baseball player, had to have a liver transplant and it was detailed in the New York times, describing where the transplant took place, tests that were administered, recovery activities, and the status of his new liver (Dubler and Kalkut 2006).
In 2007, when actor George Clooney was admitted after a motorcycle crash, 27 hospital employees were suspended after they had inappropriately accessed his medical records (Alfandre et al. 2016).
With this in mind, we must realize that we are not immune to the pitfalls that these medical care providers fell prey to. We must practice self-awareness/be consciously aware of the tendencies VIPs have towards knowing how to get their way, as well as our own propensities to enable or become starstruck. It could be charisma and charm, beauty, or a respect or intimidation factor that influences our judgement. This is where asking the questions from earlier, such as determining our motives, becomes crucial.
Minor Exceptions
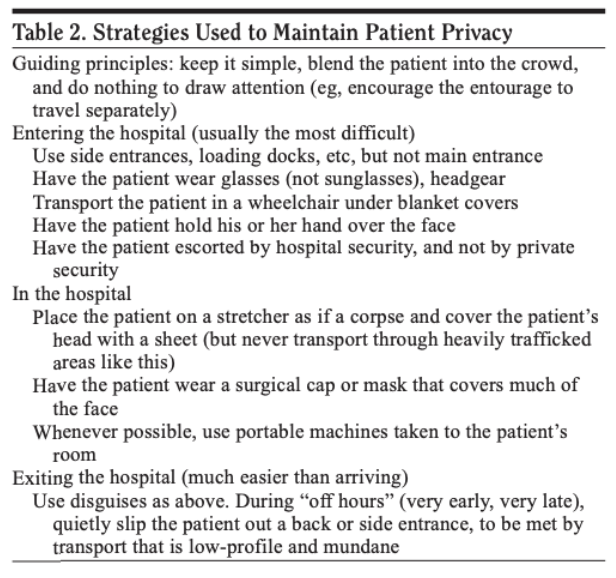
Privacy, especially for celebrity patients, can be exceptionally difficult. Medical staff must take all precautions necessary to make sure the patient is guarded from media, paparazzi, reporters, the celebrity’s entourage, or even family members who do not have permission from the patient to view their medical files. The only medical staff who should have access to their medical files should be the individuals who are directly in charge of taking care of the VIP.
Thus, it might be necessary to take extra precautions when thinking about maintaining the privacy of the VIP. One example could be the need to block out the windows to the VIP’s room in order to maintain privacy from onlookers outside their doors. This may be seen as preferential treatment, but the difference is that this is a requirement to maintain the same level of privacy for a VIP that is standard for all patients. True preferential treatment occurs when the standard boundaries of care are crossed.
Steps to Avoiding VIP Syndrome
Treat every patient the same
The best course of action to avoid VIP Syndrome is to treat every patient the same. VIPs may have a high social status outside the hospital walls, but once they enter the medical facility they should be treated with the same level of care as any other patient. Each person who comes through the doors of a medical facility deserves to be treated fairly, regardless of their societal status. The VIP status is not always the fault of the patient. There are some VIPs who expect special treatment, but there are others who want to be treated as normal human beings rather than treated based on their wealth, career, or influence. It is just as likely that it is the medical staff who place a patient in VIP status, thus giving them special treatment, even if the patient just wants to be treated like any other.
Follow all protocols
It can be tempting to bend a rule here or there for VIPs or for patients that we like. Even a willingness to bend small rules can be a slippery slope to ignoring crucial protocols. Regulations are put in place for the purpose of protecting the patient and the staff, which means cutting corners can be detrimental to all involved. Physicians should constantly ask if their judgement is being hindered by their current circumstances (Guzman et al 2011).
Communication is key
It is important to remind your staff of the protocols that are expected if/when a VIP should ever arrive seeking medical attention. Communicating expectations beforehand will decrease confusion that could cause medical mistakes or special treatment. When VIPs arrive, it might also be a good idea to reiterate those same expectations to make sure everyone is on the same page.
Be wary of accepting gifts
VIPs might be kind enough to give a gift to the staff or facility; however, accepting gifts might leave you vulnerable to scrutiny over whether ulterior motives are a factor in how you care for patients. Most of the time, it is better to respectfully deny any gifts for the protection of yourself, staff, and facility.
VIP’s Difficulty with True Connection
VIPs want to be seen as human and appreciated for who they are, not only viewed through the lens of their fame, talents, or wealth. Relationally, it is a huge turn off for them. VIPs also experience what is essentially envy towards them by family and friends. Many family and friends often feel entitled to special treatment due to the nature of their relationship with the VIP, which drives a wedge in these relationships. This unconscious envy keeps the people closest to them from celebrating the VIP for who they are as a person.
Because of this, VIPs are in a unique position of not always having a safe place to express their vulnerabilities. In fact, day to day we may not even be able to register that they are struggling; they become adept at covering it very well. It is a social veneer they basically have to put on as an act of self preservation in order to fulfill the needs of their demanding careers and relationships.
Summary
As psychiatrists, when we treat the VIP like any other person they can begin to feel both safe and secure to fall apart in front of us. This is especially true when we are in some way able to humanize ourselves in front of them. Perhaps that looks like appropriately sharing a vulnerability of our own.
As is consistent with the human experience, the VIP desires true connection, but simply has a more difficult time finding a safe place to experience it authentically.
Resources:
Alfandre, D., Clever, S., Farber, N. J., Hughes, M. T., Redstone, P., & Lehmann, L. S. (2016). Caring for 'Very Important Patients'--Ethical Dilemmas and Suggestions for Practical Management. The American journal of medicine, 129(2), 143–147. https://doi.org/10.1016/j.amjmed.2015.09.019
Groves, J. E., Dunderdale, B. A., & Stern, T. A. (2002). Celebrity Patients, VIPs, and Potentates. Primary care companion to the Journal of clinical psychiatry, 4(6), 215–223. https://doi.org/10.4088/pcc.v04n0602
Guzman, J. A., Sasidhar, M., & Stoller, J. K. (2011). Caring for VIPs: nine principles. Cleveland Clinic journal of medicine, 78(2), 90–94. https://doi.org/10.3949/ccjm.78a.10113
Acknowledgements:
This article was supported by “Mental Health Education & Research”.